Patterns are tools
The end-goal is not to force a label. The end-goal is a clinically useful interpretation that can be integrated with Raynaud history, examination, autoantibodies, organ screening, and follow-up.
A practical guide to normal, non-specific, and Cutolo systemic sclerosis capillaroscopy patterns.
Representative Pattern Cases
These complete capillaroscopy studies show how normal, non-specific, and Cutolo SSc patterns appear across multiple fields. They help calibrate pattern recognition while keeping the pattern label as only one part of the capillaroscopy interpretation.
 Normal PatternNormal Pattern: Representative Case
Normal PatternNormal Pattern: Representative Case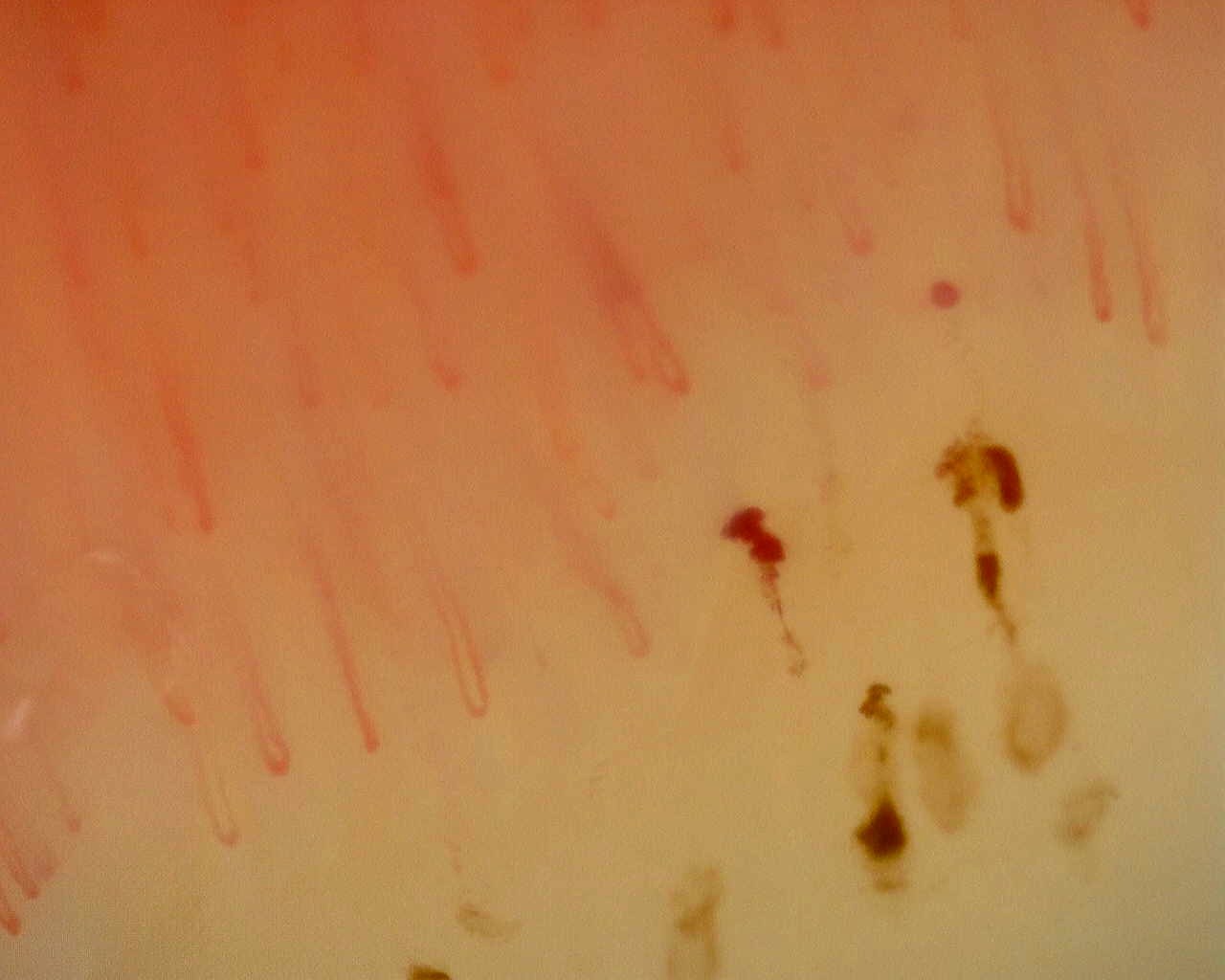 Non-Specific PatternNon-Specific Pattern: Representative Case
Non-Specific PatternNon-Specific Pattern: Representative Case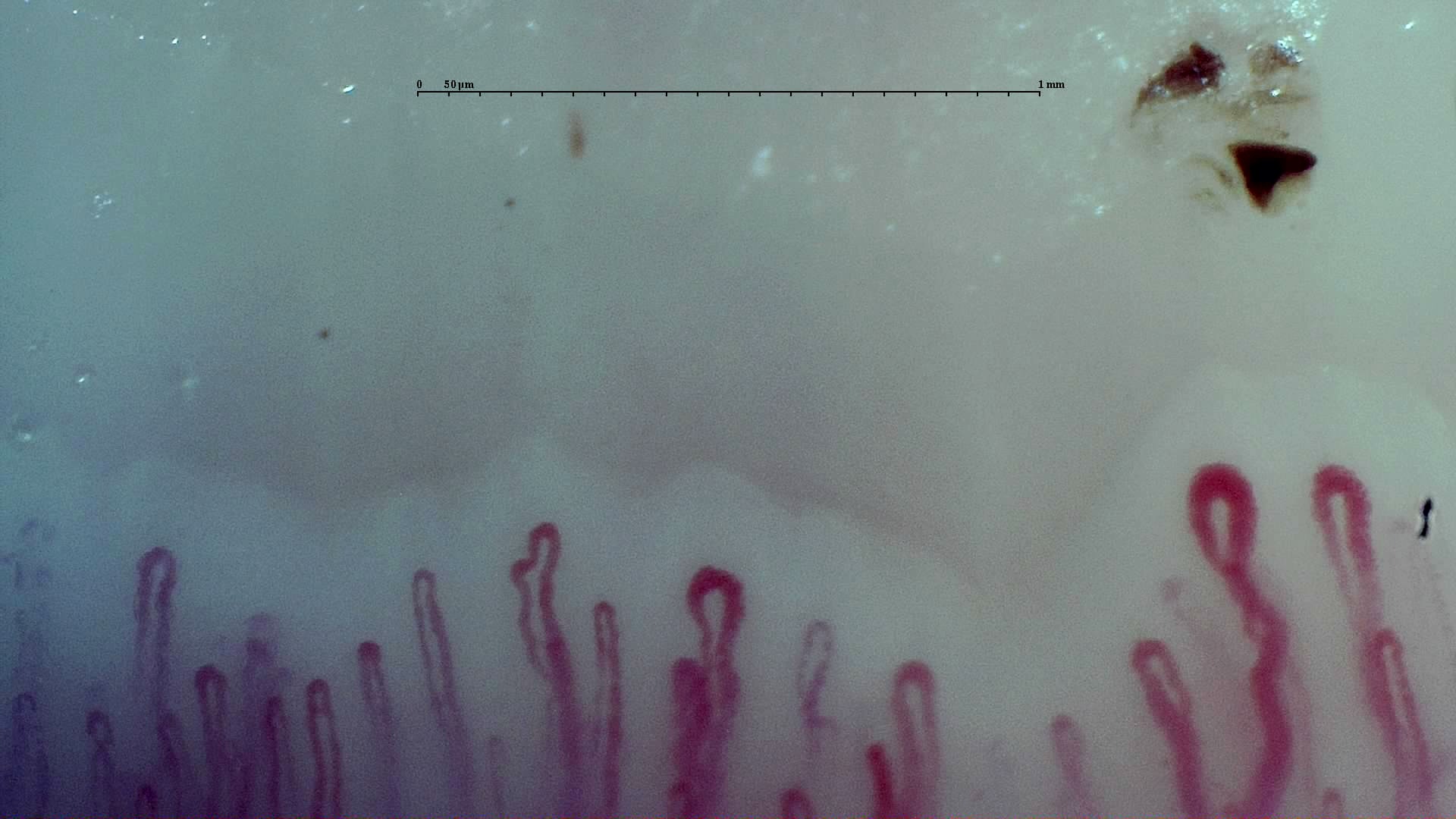 Early Cutolo SSc PatternEarly SSc Cutolo Pattern: Representative Case
Early Cutolo SSc PatternEarly SSc Cutolo Pattern: Representative Case Active Cutolo SSc PatternActive SSc Cutolo Pattern: Representative Case
Active Cutolo SSc PatternActive SSc Cutolo Pattern: Representative Case Late Cutolo SSc PatternLate SSc Cutolo Pattern: Representative Case
Late Cutolo SSc PatternLate SSc Cutolo Pattern: Representative CaseIn daily capillaroscopy, pattern recognition is a starting language, not the final answer. A useful report still has to describe image quality, capillary density, morphology, hemorrhages, avascular areas, distribution across fingers, and clinical context.
The simplest practical distinction is normal pattern, non-specific pattern, and a systemic-sclerosis-type microangiopathy. The Cutolo early-active-late scheme remains the classic way to describe scleroderma-pattern evolution in systemic sclerosis, but it is visual and partly observer-dependent.
The end-goal is not to force a label. The end-goal is a clinically useful interpretation that can be integrated with Raynaud history, examination, autoantibodies, organ screening, and follow-up.
A pattern label should be backed by visible findings: density, giant capillaries, hemorrhages, avascular areas, abnormal shapes, and whether changes repeat across several evaluable fingers.
Cutolo patterns are useful, but they are not completely objective. Borderline studies, poor image quality, mixed features, and isolated abnormalities can be interpreted differently by different readers.
Baseline
A normal pattern has an ordered distal row, preserved density, predominantly hairpin or U-shaped loops, and no coherent microangiopathic pattern.
Grey zone
A non-specific pattern contains abnormalities, but not enough structure to call it scleroderma-pattern microangiopathy.
SSc-type
A scleroderma pattern is a coherent combination of giant capillaries, hemorrhages, capillary loss, avascular areas, disorganization, and neoangiogenesis.
The Cutolo scheme is best understood as a practical description of dominant microvascular damage, not as a rigid biological sequence that every patient must follow.
Few giant capillaries and few hemorrhages, with relatively preserved capillary distribution.
Do not overcall early SSc from a single enlarged loop or one traumatic hemorrhage.
Frequent giant capillaries and hemorrhages, with moderate capillary loss and early architectural disorganization.
The active label should come from the overall field and several fingers, not from one striking capillary.
Severe capillary loss, avascular areas, disorganization, and neoangiogenesis, often with fewer typical giant capillaries.
A late pattern may look less 'giant-capillary rich' while still representing more severe microvascular damage.
These complete capillaroscopy studies show how normal, non-specific, and Cutolo SSc patterns appear across multiple fields. They help calibrate pattern recognition while keeping the pattern label as only one part of the capillaroscopy interpretation.
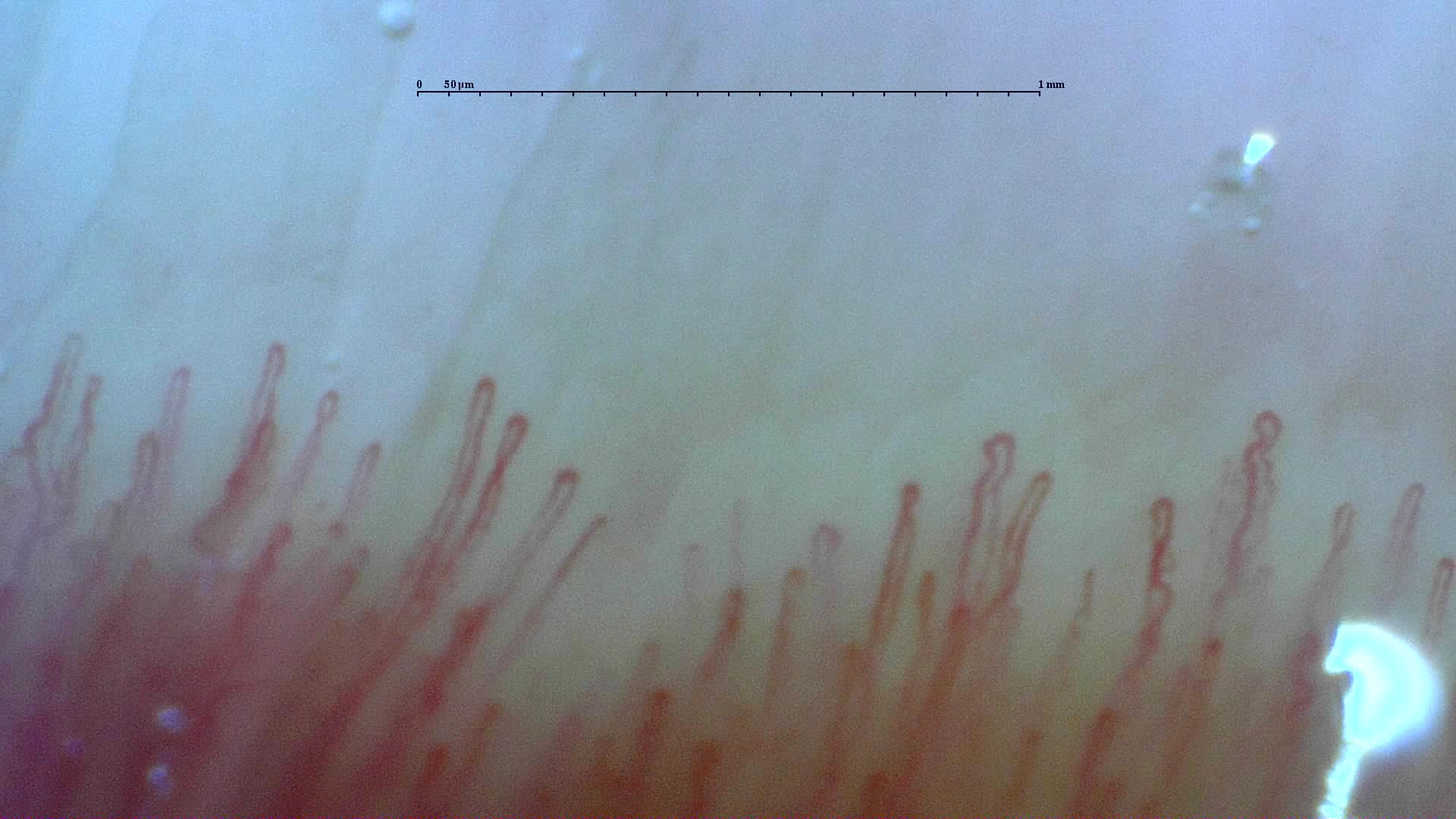
Complete capillaroscopy study with preserved density, regular morphology, and no scleroderma-pattern features.
Author: Miguel Antonio Mesa Navas
Clinical context: A normal reference study is useful for comparing density, loop morphology, and distal-row organization before judging abnormal patterns.
Capillaroscopy: The complete image set shows a regular distal row, preserved density, absent giant capillaries, and no avascular areas.
Complete capillaroscopy study with preserved density, mild morphologic changes, and hemorrhages without giant capillaries.
Author: Miguel Martín Cascón
Clinical context: This example highlights how hemorrhages or mild morphologic variation can be abnormal without forming a reproducible scleroderma pattern.
Capillaroscopy: The study shows preserved density, around 8.8 capillaries/mm, scattered dilated or tortuous loops, and hemorrhages around 0.46/mm, with no giant capillaries and no Cutolo SSc pattern.
Complete capillaroscopy study illustrating early scleroderma-pattern microangiopathy with preserved density.
Author: Borja Gracia Tello
Clinical context: In early Cutolo SSc, the descriptive label should be integrated with Raynaud history, autoantibodies, and the broader clinical assessment.
Capillaroscopy: The study shows scattered giant capillaries and limited hemorrhages while capillary density and overall architecture remain relatively preserved.
Complete capillaroscopy study with prominent giant capillaries, hemorrhages, and moderate capillary loss.
Author: Borja Gracia Tello
Clinical context: In active Cutolo SSc, pattern reading depends on the balance of giant capillaries, hemorrhages, density loss, and early disorganization across several fields.
Capillaroscopy: The study shows frequent giant capillaries and hemorrhages with reduced density and early architectural disorganization.
Complete capillaroscopy study dominated by capillary loss, architectural disorganization, and abnormal neoangiogenic shapes.
Author: Gema María Lledó Ibáñez
Clinical context: In late Cutolo SSc, fewer classic giant capillaries may coexist with more advanced microvascular damage and remodeling.
Capillaroscopy: The study shows severe capillary rarefaction, avascular areas, disorganization, and ramified or highly abnormal capillaries.