Systemic sclerosis: scleroderma pattern, criteria, and classification
In systemic sclerosis, capillaroscopy does more than help distinguish secondary Raynaud from primary Raynaud. It also makes it possible to recognize very early structural microangiopathy, integrate it with serology, and place the patient within a clinical logic that ranges from Very Early Diagnosis of Systemic Sclerosis (VEDOSS) to formal disease classification [1, 2, 3, 4, 5].
- The scleroderma pattern is one of the most useful findings when evaluating Raynaud with suspected autoimmune disease, but it should not be interpreted outside the clinical and serologic context [1, 2, 3, 4, 5].
- The combination of abnormal capillaroscopy and specific autoantibodies greatly increases the risk of progression to systemic sclerosis in patients with Raynaud [4, 5].
- The classic Maricq patterns and, especially, Cutolo's early-active-late scheme, used in most clinical studies, remain the basis of clinical practice [6, 7].
- Giant capillaries, hemorrhages, capillary loss, avascular areas, and neoangiogenesis should be interpreted together: an isolated finding carries less weight than a repeated pattern in several fingers [1, 2, 7].
- Classification reliability depends on sampling: reducing fields or analyzing only medial areas may lead to errors in assigning pattern and subtype [14].
- The scleroderma pattern is not exclusive to systemic sclerosis: a scleroderma-like pattern may occasionally be seen in dermatomyositis and other connective tissue diseases, although with different clinical meaning [1, 9].
- Although algorithms and automation contribute substantially to reducing subjectivity, they should never be interpreted without considering the whole clinical context [8, 10, 11].
Learning path
If you want to recognize when a study is compatible with a scleroderma pattern, this unit gives you the practical criteria and most frequent errors. It will then be useful to review prognosis, digital ulcers, and follow-up to understand what changes when the temporal evolution of this pattern is studied.
Why this pattern matters
Scleroderma-pattern microangiopathy is one of the earliest and most reproducible expressions of systemic sclerosis. In practice, capillaroscopy answers two different questions: whether the patient already has a microvascular phenotype compatible with the scleroderma spectrum, and which apparent phase of damage the patient is in [1, 2, 3, 7].
The technique is part of the modern diagnostic basis of systemic sclerosis because it detects structural changes before skin fibrosis or visceral involvement is clearly measurable [1, 2, 3]. Its value is especially notable in patients with Raynaud, puffy fingers, positive antinuclear antibodies (ANA), or specific autoantibodies, where capillaroscopy helps decide whether we are dealing with functional vasospasm or a connective tissue disease that is still consolidating [3, 4, 5].
It also adds value for another reason: it forces us to rethink meaning. A study with repeated giant capillaries, hemorrhages, and density loss is not interpreted the same way as a capillaroscopy with an isolated doubtful dilation. In systemic sclerosis, diagnostic strength lies in convergence of evidence pointing to the same pattern, which in turn should fit the clinical context [1, 2, 7].
| Scenario | What capillaroscopy adds | What should not be based only on this test |
|---|---|---|
| Possible Raynaud not yet diagnosed | Better separates the primary form from structural microangiopathy [1, 2, 3, 4, 5] | Labeling a connective tissue disease without integrating serology and examination |
| Suspected very early systemic sclerosis | Reinforces VEDOSS and probability of progression [4, 5] | Replacing serial clinical follow-up |
| Systemic sclerosis classification | Acts as one of the structural items in the 2013 ACR/EULAR (American College of Rheumatology / European Alliance of Associations for Rheumatology) criteria [3] | Replacing major criteria when they are absent |
| Connective tissue diseases other than systemic sclerosis | May show a scleroderma-like pattern that requires diagnostic nuance [1, 9] | Assuming that every advanced pattern equals systemic sclerosis |
Raynaud, VEDOSS, and very early phases
The most important clinical use of the scleroderma pattern begins in the patient with Raynaud. This is where capillaroscopy stops being descriptive and becomes a tool for stratifying the real risk of progression to systemic sclerosis [3, 4, 5].
Koenig's prospective study of 586 patients with Raynaud showed that specific autoantibodies and capillary microangiopathy were independent predictors of progression to systemic sclerosis. Coexistence of both increased the probability of progression, while their absence markedly lowered that risk [4]. This study remains a reference point because it showed that capillaroscopy does not merely "accompany" diagnosis: it anticipates it in a relevant proportion of patients.
VEDOSS logic later refined this scenario. In the multicenter registry published by Bellando-Randone and colleagues, progression to fulfilling ACR/EULAR criteria was overall 52.4% among patients who progressed or completed 5-year follow-up. Absence of ANA was the most protective variable: progression occurred in only 10.8% of ANA-negative patients, compared with 94.1% among those combining specific autoantibodies and puffy fingers [5]. Abnormal capillaroscopy was one of the four pillars of the model, together with ANA, specific autoantibodies, and puffy fingers.
This has a very useful practical consequence: in a patient with Raynaud, deciding "normal" versus "abnormal" is not enough. The patient must be placed on a risk gradient. Abnormal capillaroscopy in a seronegative patient without puffy fingers does not carry the same weight as the same image in someone with specific antibodies and proximal digital swelling [1, 2, 3, 4, 5].
| Baseline profile | Practical interpretation | What it usually justifies |
|---|---|---|
| Raynaud with negative ANA and normal capillaroscopy | Low risk of immediate evolution to systemic sclerosis [4, 5] | Reasonable, non-intensive clinical follow-up |
| Raynaud with positive ANA and doubtful capillaroscopic findings | Gray zone requiring caution, repetition, and context [1, 2, 5] | Clinical review and possible repetition if suspicion persists |
| Raynaud with specific autoantibodies and scleroderma pattern | High risk of progression and reclassification [4, 5] | Expanded workup, close surveillance, and assessment of early damage |
| Raynaud with puffy fingers and an abnormal pattern | Very suggestive phenotype of very early disease [3, 5] | Apply VEDOSS logic and look for incipient involvement |
What we mean by scleroderma pattern
Speaking of a scleroderma pattern does not mean pointing to a single finding. It is a constellation of changes in size, density, hemorrhages, and architecture that, when repeated in several fingers, depicts microangiopathy typical of the scleroderma spectrum [1, 2, 6, 7, 8].
The most recognizable elements are dilated capillaries and, especially, giant capillaries, hemorrhages, density loss, avascular areas, architectural disorganization, and abnormal forms or neoangiogenesis [1, 2, 7]. In practice, useful reading is not about checking boxes, but deciding whether these components form a coherent pattern and inferring its possible evolution.
Many groups use an apical diameter >20 μm to describe dilated capillaries and reserve 50 μm or more for giant capillaries [12]. At the same time, more recent reviews remind us that normal apical width may approach 25 μm depending on method and population, so context, calibration, and repetition of the finding remain decisive [13]. An isolated giant capillary may be striking; a group of giant capillaries accompanied by hemorrhages and capillary rarefaction has much greater interpretive weight [2, 8].
Vocabulary has also changed. Historical literature and some scales still speak of megacapillaries and ramified capillaries, while more recent reviews and algorithms prefer giant capillaries and abnormal shapes. In practice, these refer to the same morphologic continuum with a more updated and observer-homogeneous lexicon [1, 2, 7, 8].
It is also worth remembering that "scleroderma" does not mean "exclusive to systemic sclerosis." Scleroderma-like patterns occur in dermatomyositis, undifferentiated connective tissue disease, lupus, or rheumatoid arthritis, with differences in frequency and phase distribution. Lambova and Müller-Ladner's 2024 comparative review reinforces this idea: the advanced pattern remains much more typical of systemic sclerosis, but not every image compatible with active or late phase should be interpreted without considering the specific clinical context [9].

| Domain | What it suggests | Useful nuance |
|---|---|---|
| Giant capillaries | Typical and relatively early structural lesion [1, 2, 7, 8] | They carry more weight if multiple and accompanied by hemorrhages |
| Microhemorrhages | Active or recent microvascular damage [1, 2, 7] | Cuticle trauma or recent manipulation must be excluded |
| Density loss | Capillary rarefaction and progression of damage [1, 2, 7] | It gains value when repeatedly observed in several fields or fingers and not caused by poor technical quality |
| Avascular areas | More advanced damage and structural disruption [1, 7] | Not every empty zone in a single photograph is a clinically relevant avascular area |
| Abnormal shapes and neoangiogenesis | Disordered vascular repair attempt [1, 7, 9] | They are more significant if they coexist with capillary loss |
Maricq and Cutolo classifications
Classifications do not exist to add elegant labels, but to organize progression of microvascular damage. Maricq opened the way with a more binary reading; Cutolo refined evolution into an early-active-late sequence that remains the most used in teaching, research, and clinical follow-up [6, 7].
Maricq: the historical logic
Maricq's studies established that alternation between dilated loops and capillary loss could define microangiopathy compatible with systemic sclerosis or dermatomyositis [6]. In teaching practice, its current utility is historical and conceptual: it helps us understand that, since the 1970s, a difference was already identified between predominantly dilative forms and forms with more extensive capillary destruction.
Cutolo: the most used classification today
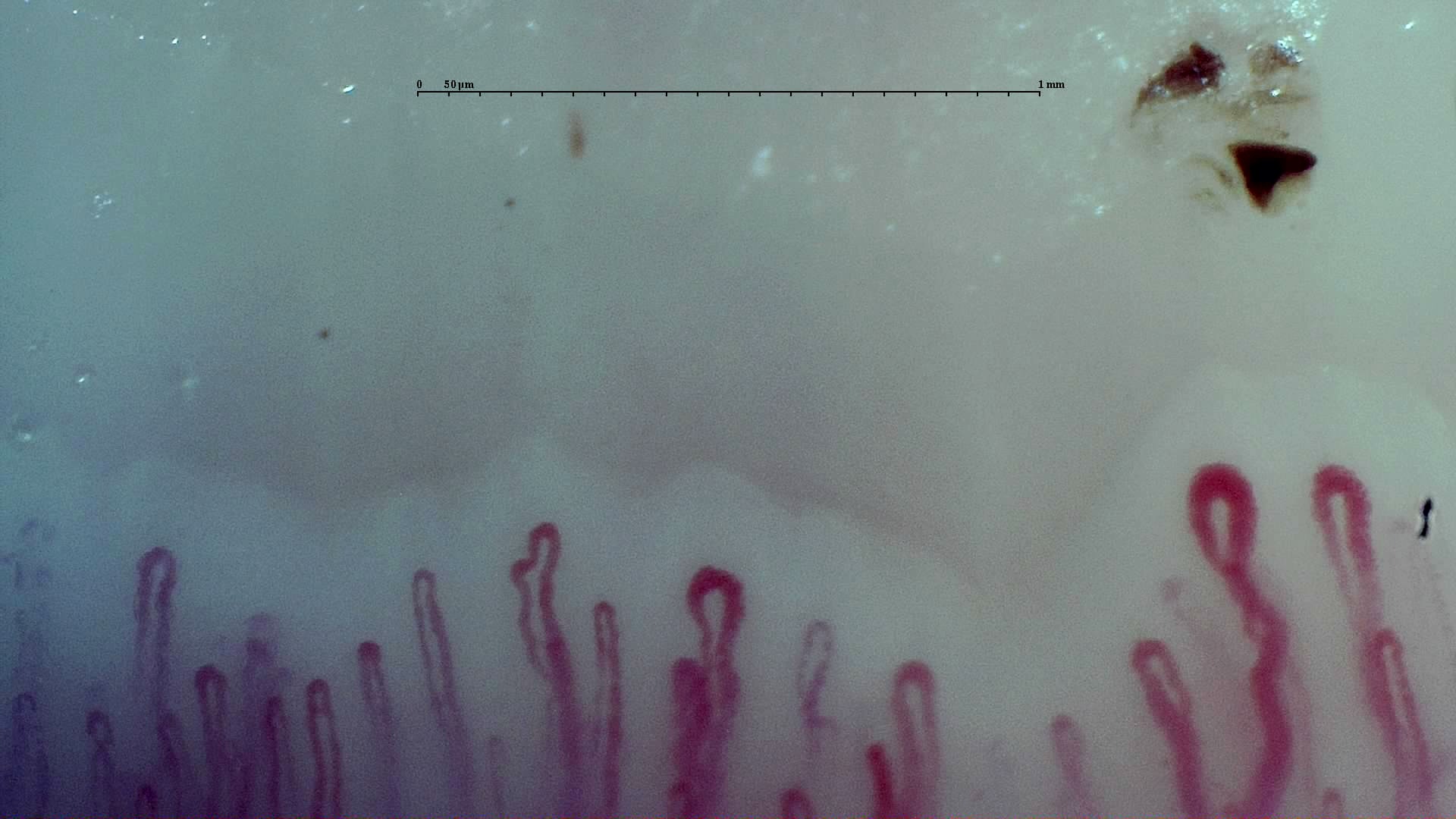
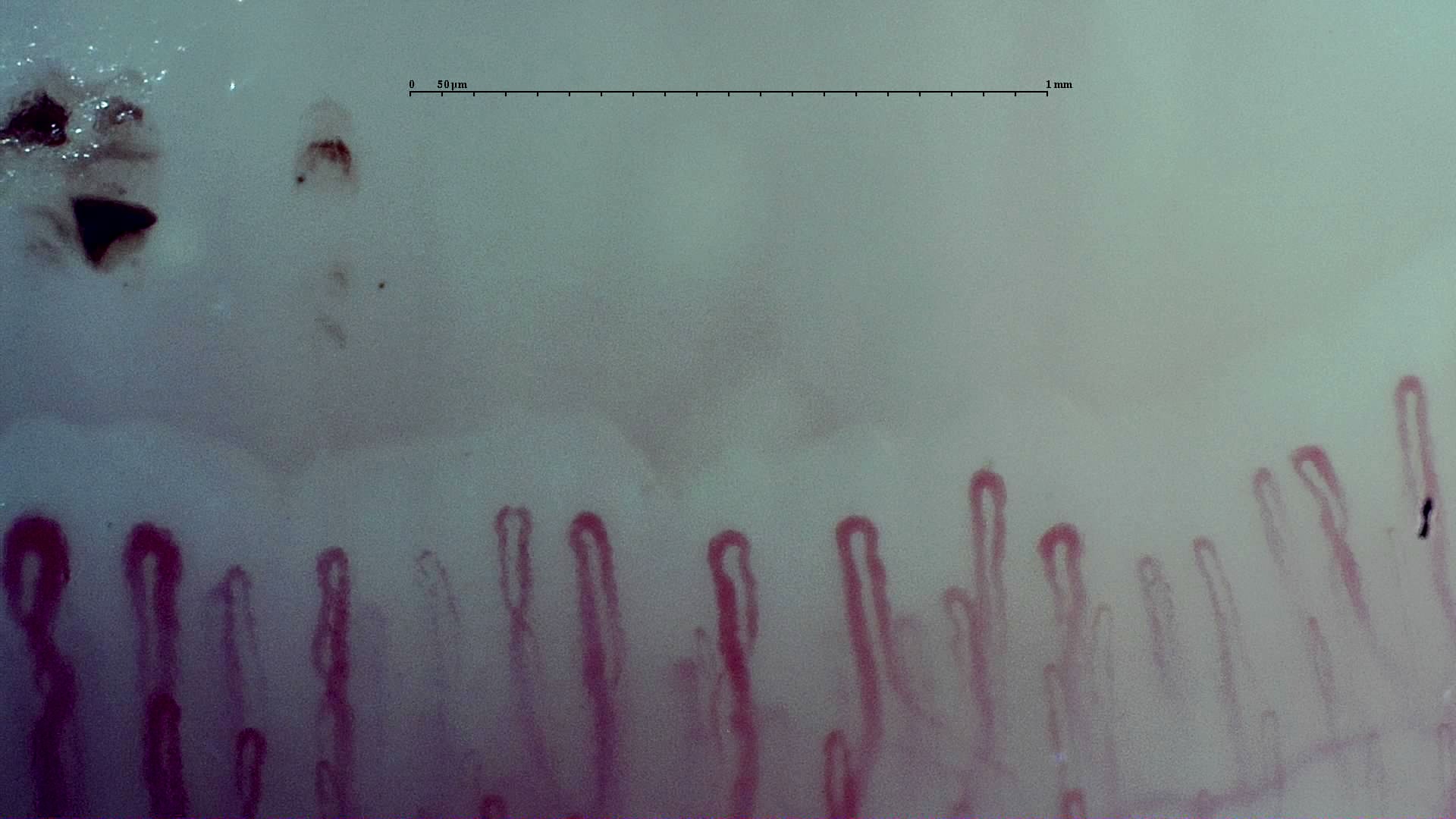
Cutolo's classification defines three phases. The early pattern shows, although infrequently, giant capillaries and hemorrhages, with preserved global architecture and no clear capillary loss. The active pattern shows frequent giant capillaries and hemorrhages, moderate capillary loss, and increasing disorganization. The late pattern combines obvious rarefaction, avascular areas, abnormal shapes, and structural disruption, with less prominence of giant capillaries [1, 7].
These categories should not be read as a perfect biological clock. "Early," "active," and "late" describe a predominant morphology, not an exact disease duration. The 2024 review on scleroderma-like patterns insists precisely on this: an active or late pattern may appear at different durations and does not automatically correspond to an identical linear chronology in every patient [9].
| Classification | Categories | What it adds today | Limitations |
|---|---|---|---|
| Maricq [6] | Forms with predominant dilation versus more destructive capillary damage | Historical and conceptual value | Less granularity for current follow-up |
| Cutolo [7] | Early, active, and late | Practical and reproducible language for clinic and research | Subjectivity linked to examiner experience; does not always reflect exact chronology |
| Cutolo pattern | Dominant findings | Practical interpretation |
|---|---|---|
| Early | Presence, although scarce, of giant capillaries and hemorrhages; preserved architecture; almost preserved density [1, 7] | Suggests already structural but still minimally destructive microangiopathy |
| Active | Frequent giant capillaries and hemorrhages, moderate capillary loss, and increasing disorganization [1, 7] | Reflects a more intense phase of vascular injury |
| Late | Obvious rarefaction, avascular areas, abnormal shapes, and severely altered architecture [1, 7] | Indicates advanced microvascular damage and is usually associated with greater clinical burden |
 A. Early
A. Early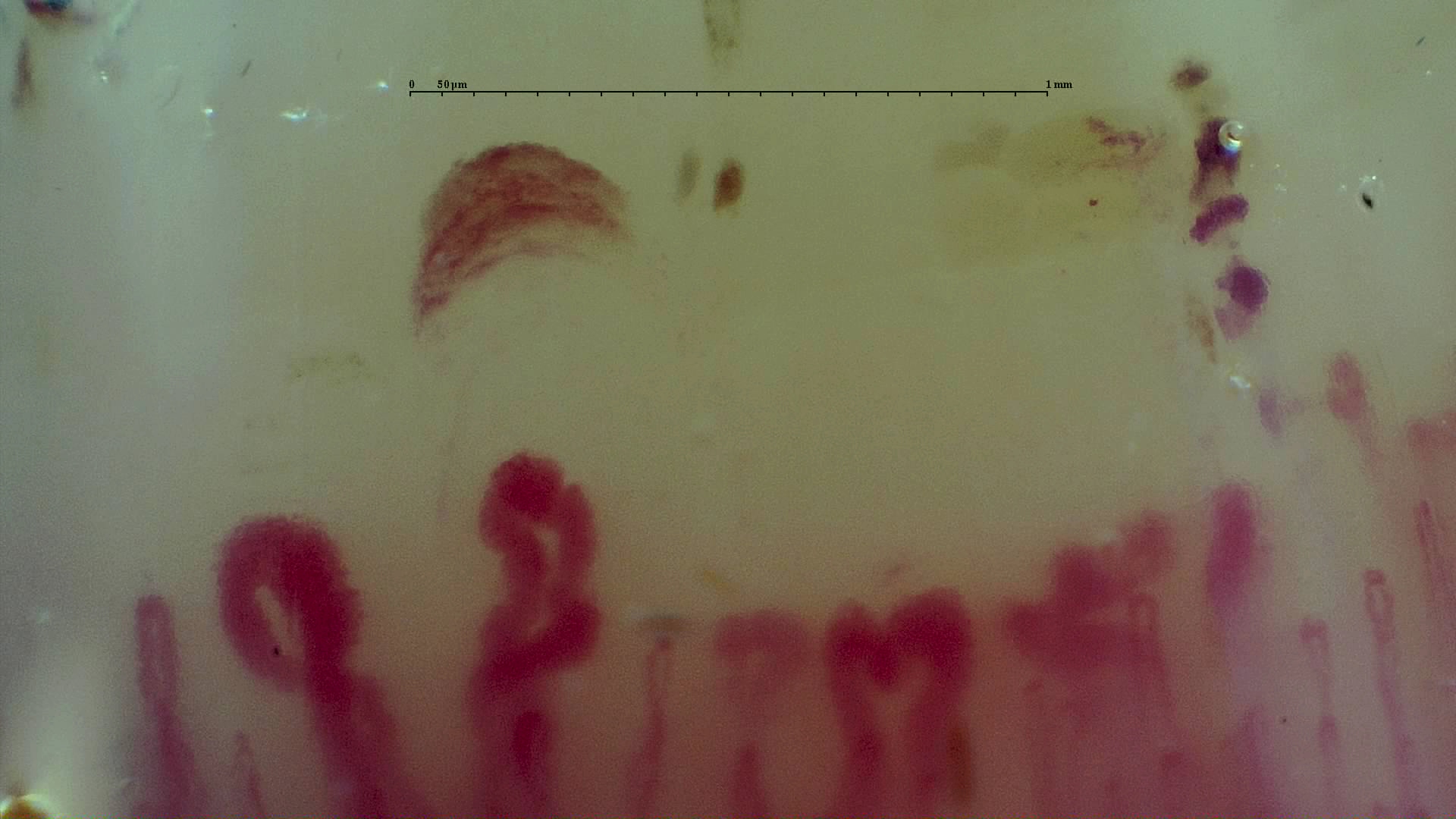 B. Active
B. Active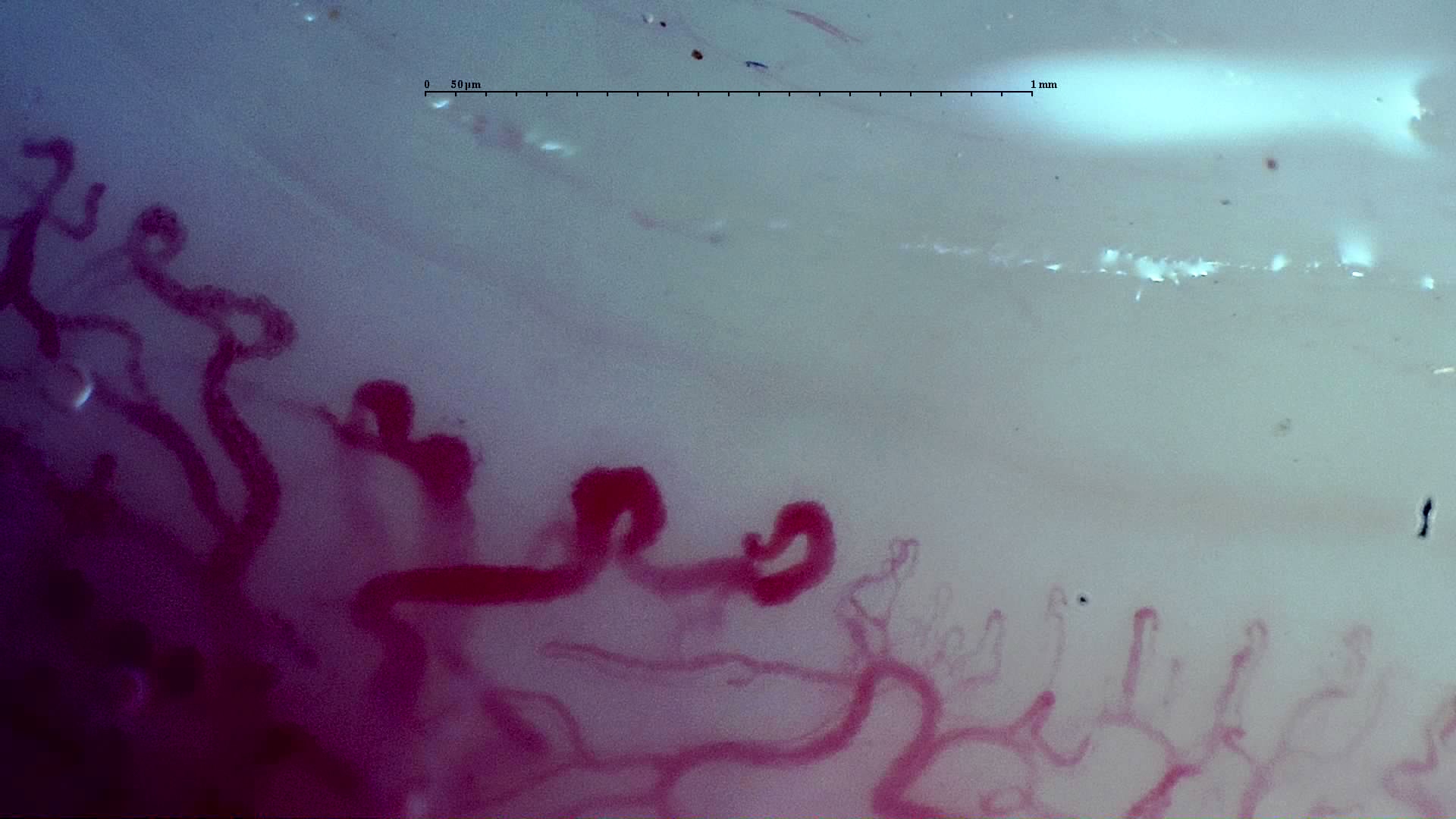 C. Late
C. LatePractical rules and automation
Interobserver variability remains one of the major problems in capillaroscopy. That is why two parallel lines of work have emerged: simple algorithms for clinical experts and quantitative or machine-learning models to reduce subjectivity [1, 2, 8, 10, 11, 14].
The Fast Track algorithm proposed by the European Alliance of Associations for Rheumatology (EULAR) group simplifies the initial decision between scleroderma and non-scleroderma patterns using a few features, especially giant capillaries, capillary loss, and abnormal morphologies [8]. Its practical value lies in reducing ambiguous vocabulary and guiding a first classification, especially in settings where not all observers have the same level of experience.
More recently, Capi-score and CAPI-Detect have attempted to translate this logic into quantitative and automated language. Capi-score starts from objectifiable metrics to discriminate disease patterns, while CAPI-Detect uses machine learning and detects additional variables with diagnostic impact [10, 11]. Both approaches are promising, but their current use is supportive: they do not yet replace clinical judgment, nor do they eliminate the need to analyze findings within each patient's clinical context.
A 2026 study on classifying the systemic sclerosis pattern introduced an important operational nuance: pattern assignment depends on the number of images studied. Compared with analysis based on 32 images (recommended), analysis with 16 images produced 26.7% disagreement and incorrectly reclassified as non-scleroderma a substantial proportion of patterns that were scleroderma-pattern; moreover, more than 30% of subtypes changed [14].
| Tool | Objective | Advantage | Limitations |
|---|---|---|---|
| Fast Track [8] | Distinguish scleroderma pattern from non-scleroderma pattern | Simple, educational, and clinically applicable | Does not completely remove reading subjectivity |
| Capi-score [10] | Classify patterns with quantitative metrics | Standardizes features that were previously more visual | Needs broad validation and homogeneous adoption |
| CAPI-Detect [11] | Improve diagnosis with machine learning | May detect variables less obvious to the human eye | Still does not replace expert reading or quality control |
| Complete sampling [14] | Preserve classification reliability | Reduces bias from omitted fields | Requires more captures and study traceability |
Frequent errors and limitations
The most common errors usually do not come from not knowing that a giant capillary exists, for example, but from overinterpreting poor images, confusing isolated findings with patterns, or extrapolating too much from a single visit.
Error 1: turning an isolated finding into a diagnosis
A striking dilation in one finger, or even a hemorrhage in a traumatic context, is not equivalent to a scleroderma pattern. Correct reading requires repeated findings in several evaluable fingers and a coherent overall structure [1, 2, 7].
Error 2: forgetting the mimics
Dermatomyositis is the major mimic of the scleroderma pattern, but not the only one. Lupus, undifferentiated connective tissue disease, or rheumatoid arthritis may show scleroderma-like patterns less frequently or with different morphologic combinations [1, 9]. Therefore, a highly abnormal capillaroscopy without an evident scleroderma skin phenotype should not automatically be identified with systemic sclerosis.
Error 3: using the classification as if it were a date
"Early" does not necessarily mean "only a few months," and "late" does not mean that the patient has had the disease for decades. Morphology identifies a stage, but speed of evolution varies between patients and diseases [1, 7, 9].
Error 4: ignoring technical quality
Poor visibility, excessive pressure, poor orientation of the distal region, or traumatized cuticle may suggest capillary loss or hemorrhages. The 2020 standardization remains relevant precisely because it emphasizes that study reproducibility depends much more on how it is acquired and reported than on adding sophisticated adjectives [2].
Short clinical cases
The following scenarios summarize how interpretation changes when similar findings are placed in different clinical contexts.
Case 1: low-risk Raynaud
A 24-year-old woman has had Raynaud since adolescence, negative ANA, no puffy fingers, and normal capillaroscopy. The image does not prove absolute benignity, but it does support a low-risk profile for systemic sclerosis at baseline [4, 5].
Case 2: Raynaud in a VEDOSS scenario
A 39-year-old patient has had Raynaud for two years, ANA 1/640, anticentromere antibodies, and puffy fingers. Capillaroscopy shows repeated giant capillaries and some hemorrhages with fairly preserved density. The pattern suggests early scleroderma microangiopathy and fits well with a VEDOSS scenario [3, 5, 7].
Case 3: advanced pattern outside the classic skin phenotype
A patient has proximal weakness, a rash compatible with dermatomyositis, and capillaroscopy with giant capillaries, abnormal shapes, and rarefaction. The image may be scleroderma-like, but the main diagnosis is not necessarily systemic sclerosis. Morphology should broaden the reasoning, not close it prematurely [1, 9].
FAQ
Does a scleroderma pattern always mean systemic sclerosis?
No. It is highly suggestive in the right context, but a scleroderma-like pattern may also be seen in dermatomyositis and other connective tissue diseases [1, 9].
In a patient with Raynaud, what carries more weight: capillaroscopy or serology?
The combination is most useful. Abnormal capillaroscopy and specific autoantibodies greatly increase progression risk compared with either finding alone [4, 5].
Do the 2013 ACR/EULAR criteria require a complete Cutolo pattern?
No. The criteria include abnormal capillaroscopy as part of the classification set, but they do not require the report to use the early-active-late label [3].
Can systemic sclerosis occur with inconclusive capillaroscopy?
Yes. Although abnormal capillaroscopy is very frequent, diagnosis remains clinical-classificatory and may require longitudinal reassessment [1, 2, 3].
What is the real utility of Fast Track?
It helps separate scleroderma patterns from non-scleroderma patterns in a simpler way, reducing some interobserver variability [8].
Glossary
- VEDOSS
- Strategy to identify very early systemic sclerosis in patients with Raynaud, ANA, puffy fingers, specific autoantibodies, and/or abnormal capillaroscopy.
- Giant capillary
- Homogeneously dilated capillary loop; the preferred term in many recent texts and equivalent to the historical megacapillary. Many studies use an operational threshold of 50 μm or more, while smaller dilations are often described above 20 μm.
- Abnormal shape
- Umbrella term for irregular capillary morphologies; in classic literature it often overlaps with ramified capillaries or branching.
- Scleroderma pattern
- Set of capillaroscopic abnormalities typical of the scleroderma spectrum, with variable combination of dilations, hemorrhages, rarefaction, and disorganization.
- Scleroderma-like pattern
- Capillary image resembling the scleroderma pattern but appearing in diseases other than systemic sclerosis.
- Avascular area
- Zone with evident capillary loss in the distal region, more suggestive of advanced microvascular damage.
References
- Smith V, Ickinger C, Hysa E, Snow M, Frech T, Sulli A, et al. Nailfold capillaroscopy. Best Pract Res Clin Rheumatol. 2023;37(1):101849. doi: 10.1016/j.berh.2023.101849. PMID: 37419757.
- Smith V, Herrick AL, Ingegnoli F, Damjanov N, De Angelis R, Denton CP, et al. Standardisation of nailfold capillaroscopy for the assessment of patients with Raynaud's phenomenon and systemic sclerosis. Autoimmun Rev. 2020;19(3):102458. doi: 10.1016/j.autrev.2020.102458. PMID: 31927087.
- van den Hoogen F, Khanna D, Fransen J, Johnson SR, Baron M, Tyndall A, et al. 2013 classification criteria for systemic sclerosis: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Ann Rheum Dis. 2013;72(11):1747-1755. doi: 10.1136/annrheumdis-2013-204424. PMID: 24092682.
- Koenig M, Joyal F, Fritzler MJ, Roussin A, Abrahamowicz M, Boire G, et al. Autoantibodies and microvascular damage are independent predictive factors for the progression of Raynaud's phenomenon to systemic sclerosis: a twenty-year prospective study of 586 patients, with validation of proposed criteria for early systemic sclerosis. Arthritis Rheum. 2008;58(12):3902-3912. doi: 10.1002/art.24038. PMID: 19035499.
- Bellando-Randone S, Del Galdo F, Lepri G, Minier T, Huscher D, Furst DE, et al. Progression of patients with Raynaud's phenomenon to systemic sclerosis: a five-year analysis of the European Scleroderma Trial and Research group multicentre, longitudinal registry study for Very Early Diagnosis of Systemic Sclerosis (VEDOSS). Lancet Rheumatol. 2021;3(12):e834-e843. doi: 10.1016/S2665-9913(21)00244-7. PMID: 38287630.
- Maricq HR, Spencer-Green G, LeRoy EC. Skin capillary abnormalities as indicators of organ involvement in scleroderma (systemic sclerosis), Raynaud's syndrome and dermatomyositis. Am J Med. 1976;61(6):862-870. doi: 10.1016/0002-9343(76)90410-1. PMID: 1008072.
- Cutolo M, Pizzorni C, Tuccio M, Burroni A, Craviotto C, Basso M, et al. Nailfold videocapillaroscopic patterns and serum autoantibodies in systemic sclerosis. Rheumatology (Oxford). 2004;43(6):719-726. doi: 10.1093/rheumatology/keh156. PMID: 15026581.
- Smith V, Vanhaecke A, Herrick AL, Distler O, Guerra MG, Denton CP, et al. Fast track algorithm: How to differentiate a "scleroderma pattern" from a "non-scleroderma pattern". Autoimmun Rev. 2019;18(11):102394. doi: 10.1016/j.autrev.2019.102394. PMID: 31520797.
- Lambova SN, Müller-Ladner U. "Scleroderma" and "Scleroderma-like" capillaroscopic pattern-differences and similarities. Curr Rheumatol Rev. 2024;20(3):304-316. doi: 10.2174/0115733971265291231212045931. PMID: 38807470.
- Gracia Tello BDC, Sáez Comet L, Lledó G, Freire Dapena M, Mesa MA, Martín-Cascón M, et al. Capi-score: a quantitative algorithm for identifying disease patterns in nailfold videocapillaroscopy. Rheumatology (Oxford). 2024;63(12):3315-3321. doi: 10.1093/rheumatology/keae197. PMID: 38530791.
- Lledó-Ibáñez GM, Sáez Comet L, Freire Dapena M, Mesa Navas M, Martín Cascón M, Guillén Del Castillo A, et al. CAPI-Detect: machine learning in capillaroscopy reveals new variables influencing diagnosis. Rheumatology (Oxford). 2025;64(6):3667-3675. doi: 10.1093/rheumatology/keaf073. PMID: 39918978.
- Kubo S, Tanaka Y. Usefulness of nailfold videocapillaroscopy for systemic sclerosis. Inflamm Regen. 2016;36:5. doi: 10.1186/s41232-016-0001-x. PMID: 29259678.
- Herrick AL, Dinsdale G, Murray A. New perspectives in the imaging of Raynaud's phenomenon. Eur J Rheumatol. 2020;7(Suppl 3):S212-S221. doi: 10.5152/eurjrheum.2020.19124. PMID: 33164735.
- Guillén del Castillo A, Lledó-Ibáñez GM, Sáez Comet L, Freire Dapena M, Mesa Navas M, Martín Cascón M, et al. Value of nailfold capillaroscopy in the classification of the systemic sclerosis pattern. Med Clin (Barc). 2026;166:107426. doi: 10.1016/j.medcli.2026.107426. PMID: 42013567.