Nailfold microcirculation: anatomy, physiology, and baseline findings
To interpret a capillaroscopic image, it is essential to understand which part of the microcirculation is being visualized, how erythrocytes flow through the capillary loop, and which variations may still be compatible with normality. The anatomical and physiological basis helps avoid two common errors: underestimating specific findings and overdiagnosing nonspecific changes [1, 2, 3].
- Capillary density is one of the most robust parameters, although it is influenced by several modifiers [1, 4, 5].
- Giant capillaries and diffuse capillary loss are much more specific than many other capillaroscopic findings [2, 3, 7].
- Scleroderma microangiopathy reflects endothelial damage, inefficient repair, and disorganized angiogenesis, not vasospasm alone [2, 6].
- Cardiovascular factors and other diseases can alter capillary morphology; for that reason, physiology must always be read together with the clinical context [7, 8].
Visible anatomy
The first objective is to recognize the elementary anatomical unit, understand why the nailfold region shows the longitudinal loop, and know which anatomical variations may be normal.
Which part of the microcirculation is observed
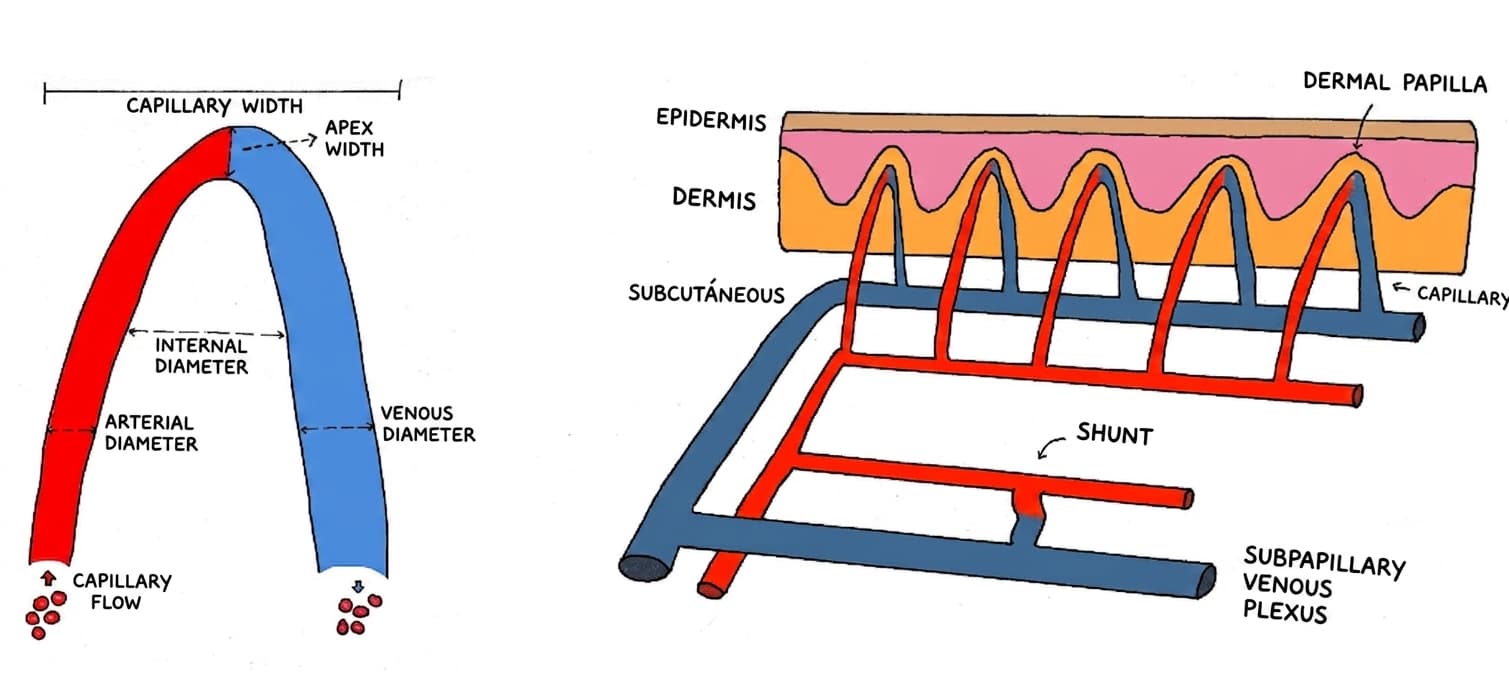
Cutaneous microcirculation includes terminal arterioles, capillaries, and postcapillary venules. Nailfold capillaroscopy mainly examines the distal row of capillary loops, where an afferent limb ascends, turns at the apex, and descends as the efferent limb. Because these loops are almost parallel to the skin surface, loop length, diameter, and density can be measured much more clearly than in other skin areas [1, 2].
| Element | Meaning in the image | Why it matters |
|---|---|---|
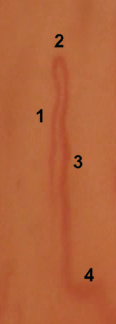
| Afferent limb | Arterial segment ascending toward the apex | Its caliber and regularity help assess dilation and asymmetry [1, 2] |
| Apex or loop | Turning point of the capillary | This is where apical diameter is measured and giant capillaries are recognized [1, 2] |
| Efferent limb | Descending venous segment | It is usually slightly wider; marked changes may reflect structural damage [1, 2] |
| Distal row | Capillaries aligned next to the cuticle in the nailfold region | This is the reference line for counting capillary density per millimeter [1, 7] |
What is normal and why there is no single number
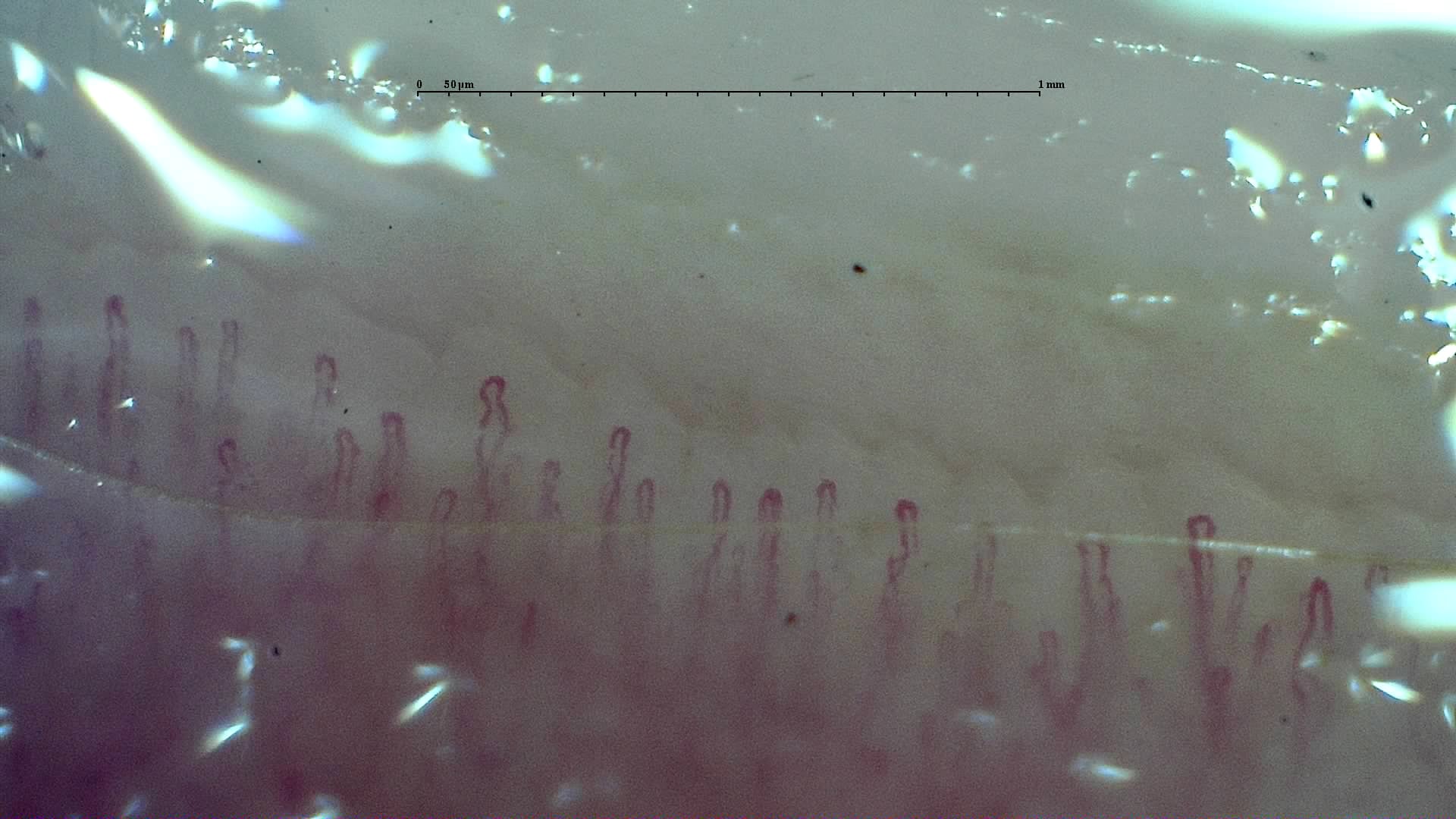
In healthy adults, one usually expects an orderly distal row, hairpin-shaped loops, and a global density of approximately 7-12 capillaries per millimeter; however, normality is not a universal number. In healthy volunteers, mild abnormalities are frequent: 67% had morphological changes, 48% had isolated hemorrhages, and only 15% showed no deviation in any finger [3].
Two nuances are crucial. First, skin phototype modifies how many capillaries can be visualized: in healthy adults, median density decreased from 8.13 cap/mm in phototype III to 4.53 cap/mm in phototype VI [4]. Second, in pediatric populations, density also varies with pigmentation, and fifth fingers show fewer capillaries than other fingers, so applying the same threshold to everyone is incorrect [5].
Findings that deserve more attention
- Giant capillaries, also known as megacapillaries.
- Diffuse density loss in the distal row.
- Hemorrhages not attributable to trauma, also known as microhemorrhages.
- Abnormal shapes, also known as ramifications.
The opposite also matters: isolated tortuosity, small abnormal shapes, or sparse hemorrhages may appear in healthy people and should not be overinterpreted when no other significant findings are present [2, 3].
Physiology and basic interpretation
Although videocapillaroscopy reflects a dynamic physiology, it is interpreted through morphological and size changes in capillaries. These changes indirectly reflect alterations in blood flow, transcapillary exchange, and the endothelial response to different insults. For example, a pathological hemorrhage is the visible expression of increased capillary inflow and/or endothelial damage that has ruptured the vessel wall and produced extravasation into the extravascular space.
Physiology of exchange and flow
The capillary network is a slow-flow system designed for the exchange of gases, water, and solutes. Functional density depends on perfusion and microvascular recruitment, whereas structural density depends on the number of visible loops in the distal row. This point is essential: functional change may precede structural injury, but clinical capillaroscopy focuses mainly on accumulated structural damage [2, 7].
| Parameter | What it expresses | Practical interpretation |
|---|---|---|
| Capillary density | Number of distal loops per mm | Good structural marker; caution is required with phototype and finger [1, 4, 5] |
| Apical diameter | Dilation of the loop | Marked enlargement supports microangiopathy; context defines specificity [1, 2] |
| Hemorrhages | Focal erythrocyte extravasation | May result from trauma, but repeated hemorrhages associated with giant capillaries carry more clinical weight [2, 3] |
| Abnormal shapes or ramifications | Attempted repair or neoangiogenesis | More informative when they coexist with density loss [2, 6] |
Determinants of heterogeneity between fingers and people
- Skin phototype and degree of pigmentation [4, 5].
- Examined finger, with lower expected density in fifth fingers [5].
- Microtrauma from manicure, onychophagia, or repetitive manual activity [1, 2].
- Cardiovascular and metabolic factors, which may be associated with tortuosities, hemorrhages, or density loss [7, 8].
Microvascular injury and specificity
The advanced key is to connect physiology with pathology: how sustained endothelial injury generates the findings later interpreted as specific or nonspecific microvascular damage.
From endothelial injury to the capillaroscopic pattern
In systemic sclerosis, small-vessel vasculopathy precedes fibrosis and is associated with endothelial dysfunction, apoptosis, imbalance between vasodilator and vasoconstrictor mediators, platelet activation, and ineffective angiogenic repair [2, 6]. In imaging, this process translates into early dilation, hemorrhages, loss of loops, and later abnormal shapes, reflecting insufficient and disorganized neoangiogenesis [2, 6].
| Finding | Probable biological basis | Indicative degree of specificity |
|---|---|---|
| Giant capillary or megacapillary | Marked dilation after endothelial injury and wall alteration Persistently increased capillary inflow | High for the scleroderma spectrum when repeated [2, 3] |
| Hemorrhage | Vascular fragility or microtrauma | Intermediate; gains value when it coexists with giant capillaries [2, 3] |
| Diffuse capillary loss | Vascular destruction and failed repair | High when extensive and persistent [2, 6, 7] |
| Extensive abnormal shapes | Disorganized reparative neoangiogenesis | Intermediate-high within advanced patterns [2, 6] |
| Isolated tortuosity | Anatomical variation, mechanical stress, or vascular factors | Low [3, 7, 8] |
Why nonspecific findings matter
More recent literature shows associations between capillaroscopic abnormalities and cardiovascular disease, psoriasis, or conventional risk factors. In a single-center study of 402 subjects, all analyzed morphological abnormalities were associated with cardiovascular risk factors, with especially high odds ratios for abnormal shapes and dilated capillaries [8].
Capillaroscopy checklist
- Confirm that the distal row is well focused and there is no pressure-induced collapse.
- Attempt a capillary count across the maximum number of millimeters of the nailfold bed.
- Review the patient's baseline characteristics, including comorbidities, personal history, and phototype [4, 5].
- Identify trauma or artifact.
- Look for combined capillaroscopic findings, not just isolated abnormalities [2, 3].
FAQ
Am I seeing the capillary itself or the blood inside it?
In clinical practice, what is visible is mainly the intracapillary blood column. This is why illumination, focus, and pressure change the appearance of the image so much [1, 2].
Should all fingers have the same density?
No. Even in healthy people there is variation between fingers; fifth fingers usually show fewer capillaries than the others [5].
Is an isolated hemorrhage pathological?
Not necessarily. It may be related to microtrauma. Its value increases when it is repeated, multiple, or accompanied by giant capillaries and density loss [2, 3].
Is tortuosity a strong sign of autoimmune disease?
No. It is one of the least specific findings and is frequent in healthy populations [3].
Can I use the same density cutoff in all phototypes?
No. Visualization decreases with greater skin pigmentation, which can reduce the visible count without implying disease [4, 5].
Glossary
- Capillary density
- Number of visible capillary loops in the distal row per linear millimeter.
- Giant capillary
- A homogeneously dilated capillary; this is the preferred term in many recent texts and corresponds to the historical term megacapillary. In videocapillaroscopy, it is usually reserved for apical diameters of 50 μm or more, whereas smaller dilations are usually described above 20 μm.
- Abnormal shape
- Umbrella term for irregular capillary morphologies; in older texts, it often overlaps with branched capillaries or ramifications.
- Avascular area
- Visible loss of capillaries in the distal row; many series use the absence of two or more consecutive capillaries as the operational definition [7].
- Neoangiogenesis
- Formation of new vessels; in capillaroscopy, it usually appears as abnormal shapes or bushy capillaries.
- Phototype
- Skin classification that influences capillary visibility and should be considered before setting quantitative thresholds [4].
References
- Smith V, Herrick AL, Ingegnoli F, Damjanov N, De Angelis R, Denton CP, et al. Standardisation of nailfold capillaroscopy for the assessment of patients with Raynaud's phenomenon and systemic sclerosis. Autoimmun Rev. 2020;19(3):102458. doi: 10.1016/j.autrev.2020.102458. PMID: 31927087.
- Smith V, Ickinger C, Hysa E, Snow M, Frech T, Sulli A, et al. Nailfold capillaroscopy. Best Pract Res Clin Rheumatol. 2023;37(1):101849. doi: 10.1016/j.berh.2023.101849. PMID: 37419757.
- Hoerth C, Kundi M, Katzenschlager R, Hirschl M. Qualitative and quantitative assessment of nailfold capillaries by capillaroscopy in healthy volunteers. Vasa. 2012;41(1):19-26. doi: 10.1024/0301-1526/a000159. PMID: 22247056.
- Bairwa D, Kavadichanda CG, Dunga S, Mathew A, Aishwarya G, Gayathri MS, et al. Effect of skin phototype on quantitative nailfold capillaroscopy. J Scleroderma Relat Disord. 2022;7(3):197-203. doi: 10.1177/23971983221102688. PMID: 36211202.
- Bergkamp SC, Smith V, Kuijpers TW, Cutolo M, van den Berg JM, Schonenberg-Meinema D. Correlations between capillary density and degree of skin pigmentation in healthy children analysed by nailfold video capillaroscopy. Quant Imaging Med Surg. 2023;13(6):3938-3947. doi: 10.21037/qims-22-993. PMID: 37284120.
- Fioretto BS, Rosa I, Matucci-Cerinic M, Romano E, Manetti M. Current Trends in Vascular Biomarkers for Systemic Sclerosis: A Narrative Review. Int J Mol Sci. 2023;24(4):4097. doi: 10.3390/ijms24044097. PMID: 36835506.
- Lim MWS, Setjiadi D, Dobbin SJH, Lang NN, Delles C, Connelly PJ. Nailfold video-capillaroscopy in the study of cardiovascular disease: a systematic review. Blood Press Monit. 2023;28(1):24-32. doi: 10.1097/MBP.0000000000000624. PMID: 36281701.
- Álvarez Andrés E, de Miguel E, García de Yébenes MJ, Carmona L, Gómez Miranda C, Collado Ramos P, et al. Relationship between nailfold videocapillaroscopic findings and cardiovascular risk factors. Microvasc Res. 2024;154:104693. doi: 10.1016/j.mvr.2024.104693. PMID: 38701966.