Normal capillaroscopy: variability, artifacts, and the limits of normality
Recognizing a normal capillaroscopy requires more than confirming that density falls within the range considered preserved. Normality depends on the global pattern, biological context, technical quality, and frequency of isolated abnormalities; therefore, the boundary between normal and nonspecific must be drawn cautiously and with standardized language [1, 2, 3, 4, 5, 6].
- A normal study combines orderly architecture, preserved density, and absence of a coherent microangiopathic pattern; an isolated abnormality is not enough by itself [1, 2, 3].
- Classic adult density ranges are useful as an initial reference, but they cannot be applied without nuance to every skin phototype, age group, and finger [2, 3, 4, 7].
- Tortuosities, scarce hemorrhages, or isolated abnormal shapes may be seen in healthy people and should be separated from repeated or combined patterns [3, 11, 12].
- Manicure, local trauma, skin phototype, and cardiovascular factors can impair visualization or generate nonspecific findings [4, 8, 9, 10].
- Routine capillaroscopy remains mainly morphological: description of flow and tissue background provides context, but it is less standardized than density or diameter [1, 2].
What defines a normal pattern
Clinically useful normality does not mean geometric perfection. It means absence of a structural microangiopathy pattern and predominance of findings compatible with physiological variation or isolated, low-specificity changes.
Before calling a study normal, make sure the image is evaluable and the distal row is clearly identified. It will then be easier to move to semiology and reporting to describe those findings with reproducible language and later apply them to indications and clinical utility.
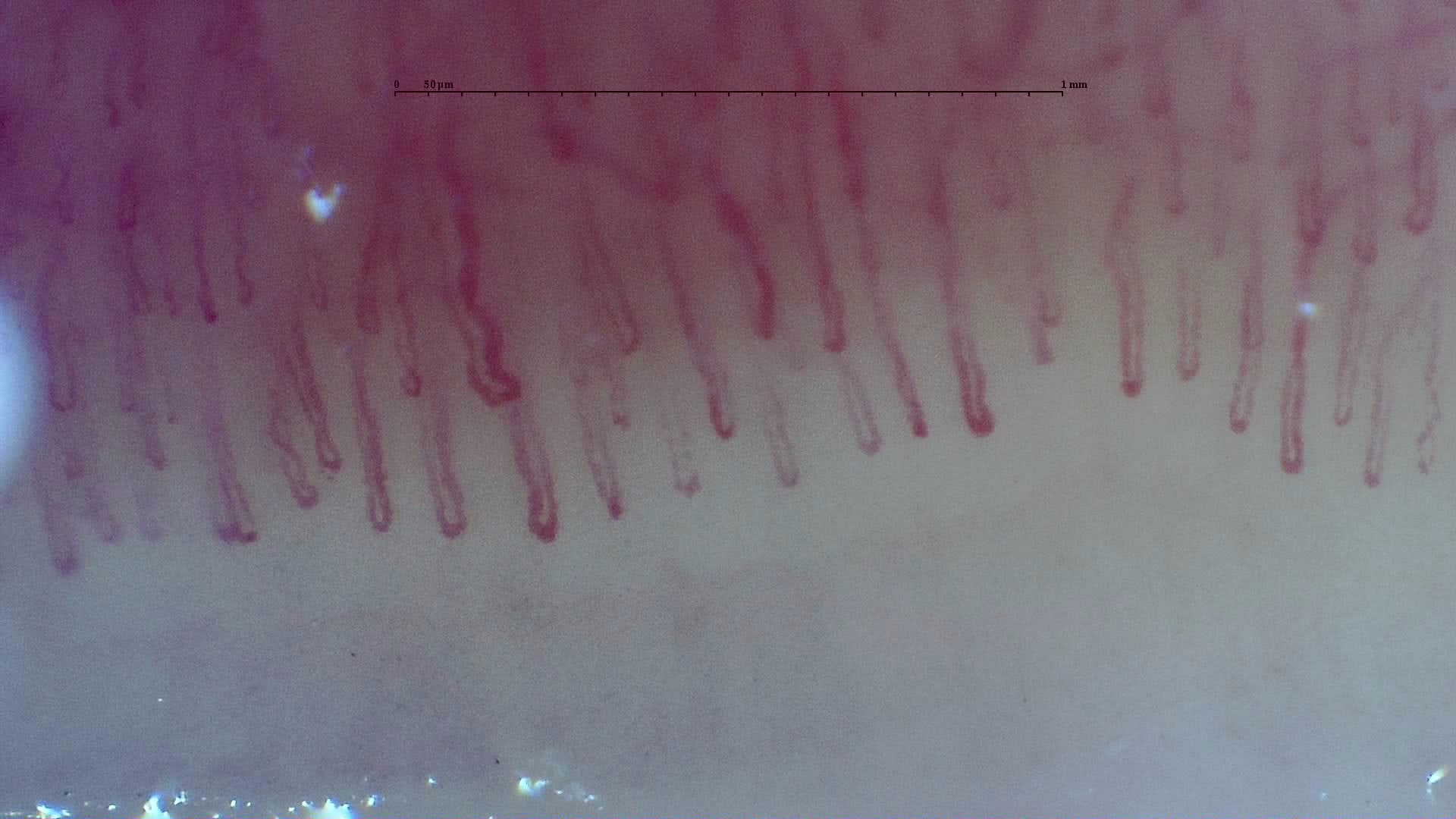
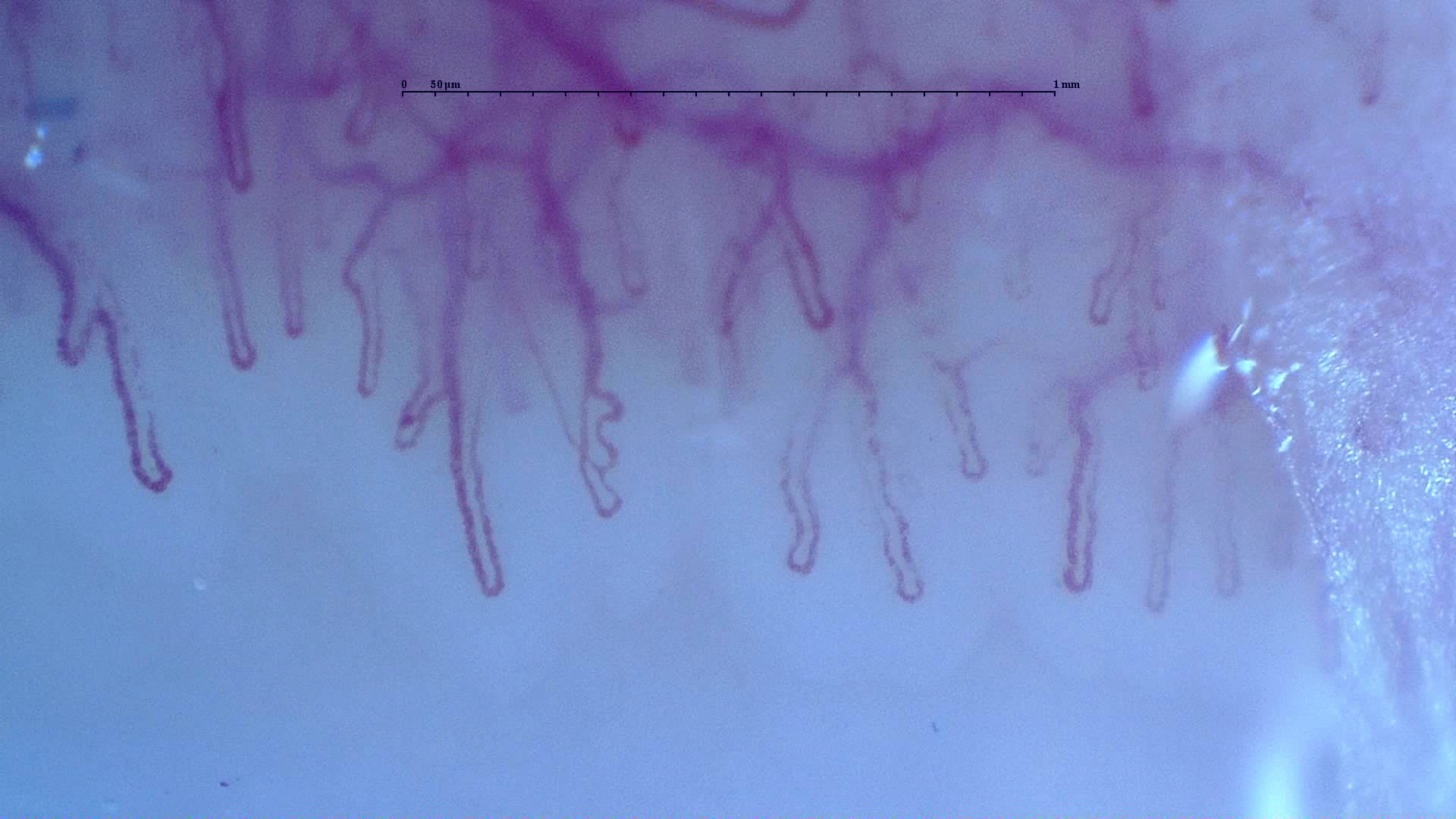
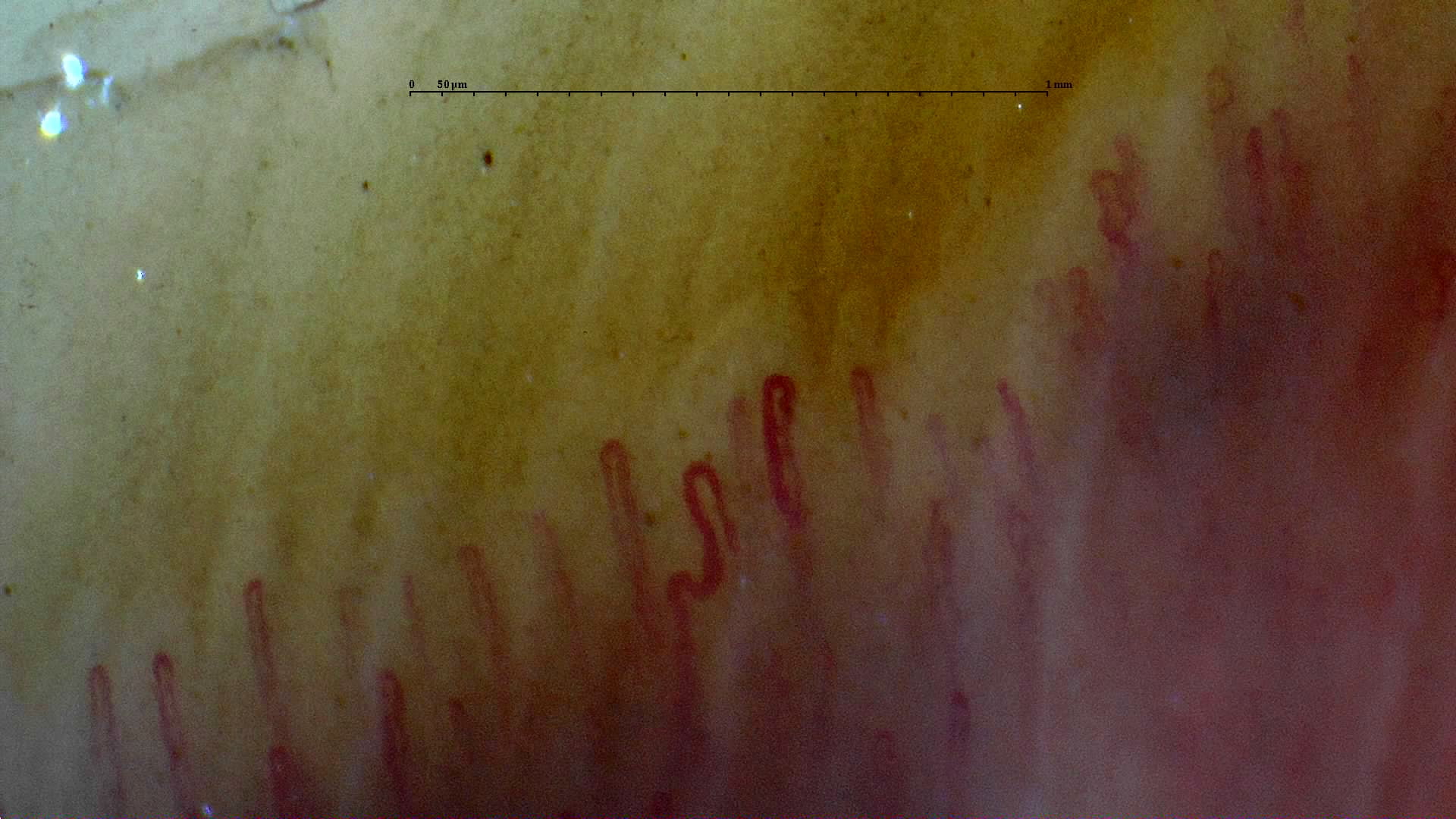
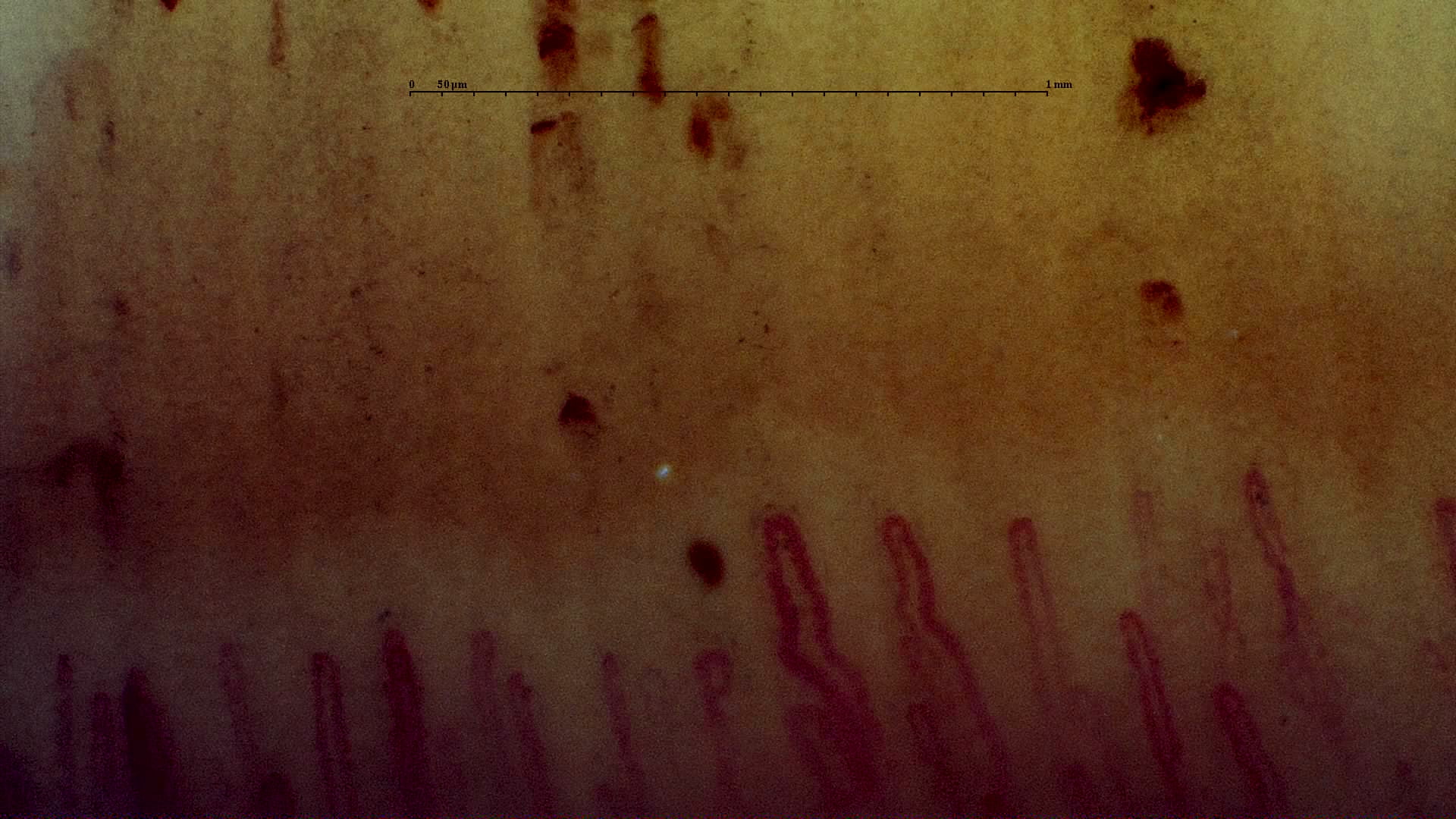
Recent methodological reviews and standardization documents converge on a simple idea: a normal study should show a recognizable distal row, a relatively orderly "comb-like" arrangement, predominantly hairpin or inverted "U" capillaries, and absence of giant capillaries, diffuse capillary loss, or repeated non-traumatic hemorrhages [1, 2]. When mild abnormalities appear, their diagnostic weight depends on their frequency, their distribution across fingers, and whether they form a coherent pattern [1, 2, 3].
| Parameter | Expected in a normal study | Warning sign |
|---|---|---|
| Global architecture | Identifiable distal row and relatively parallel organization [1, 2] | Diffuse disorganization or clear loss of the first row |
| Density | Compatible with finger-specific references and the patient's context; in healthy adults it usually lies near the classic 7-12 capillaries/mm range, but there is no universal threshold [1, 2, 3, 4] | Persistent multi-finger reduction not explained by skin phototype, age, or technique |
| Predominant morphology | Hairpin, inverted "U", or mildly tortuous loops [3, 5, 6] | Repeated loss of apical convexity, giant capillaries, or extensive abnormal shapes |
| Hemorrhages | Absent or scarce and plausibly traumatic [1, 2, 3] | Multiple recent hemorrhages associated with dilations or capillary loss |
| Conclusion | Normal or with isolated nonspecific abnormalities | Structured microangiopathic pattern |
In a cohort of 100 healthy subjects, Ingegnoli et al. described an overall pattern compatible with normality even when some morphological variants coexisted. In that series, median density was 7 capillaries per millimeter, with mean length of 207 microns, total diameter of 39 microns, and apical diameter of 17 microns [3]. These values help orientation, but they should not be treated as rigid cutoffs or extrapolated without qualification to every skin phototype or age group [3, 4, 7].
Parameters worth describing
The safest way to report a normal study is to review the same minimum set of domains every time and state clearly when a finding is physiological, nonspecific, or frankly suspicious.
Density and distribution
Capillary density remains the most robust structural parameter, but its interpretation requires context. Recent recommendations place it at the center of the report because it is more reproducible than many morphological descriptors [1, 2]. Even so, the number of visible capillaries decreases with darker skin phototypes in quantitative studies of healthy adults, and it also changes with pediatric age and with the finger examined [4, 7].
| Domain | How to describe it | Clinical nuance |
|---|---|---|
| Density | Number of evaluable distal loops per mm, ideally across several fingers [1, 2] | A borderline isolated value is not enough to diagnose microangiopathy |
| Apical diameter | Presence or absence of striking dilations and, when appropriate, apical measurement [1, 2, 3] | Precise measurement depends on correct calibration and focus |
| Morphology | Predominance of hairpin/inverted "U" loops versus tortuous or abnormal variants [3, 5, 6] | Isolated morphology is less reproducible than density or diameter |
| Hemorrhages | Number, distribution, and traumatic plausibility | Trauma, nail biting, or manicure should be separated from true microvascular damage [1, 8] |
| Subpapillary venous plexus | Visible or not visible; if prominent, describe it as context rather than as a specific lesion | It may be seen in healthy individuals, so it does not define pathology by itself [11] |
Normal morphology versus abnormal morphology
The European Alliance of Associations for Rheumatology (EULAR) microcirculation group addressed this problem specifically: which morphologies can still be considered normal and which should be labeled abnormal. In a pilot study and a subsequent exercise assessing endpoint reliability, simple definitions improved observer agreement, although overall agreement remained only moderate and depended strongly on whether the capillary was truly classifiable [5, 6]. The practical implication is clear: use simple categories and avoid overdescribing doubtful shapes.
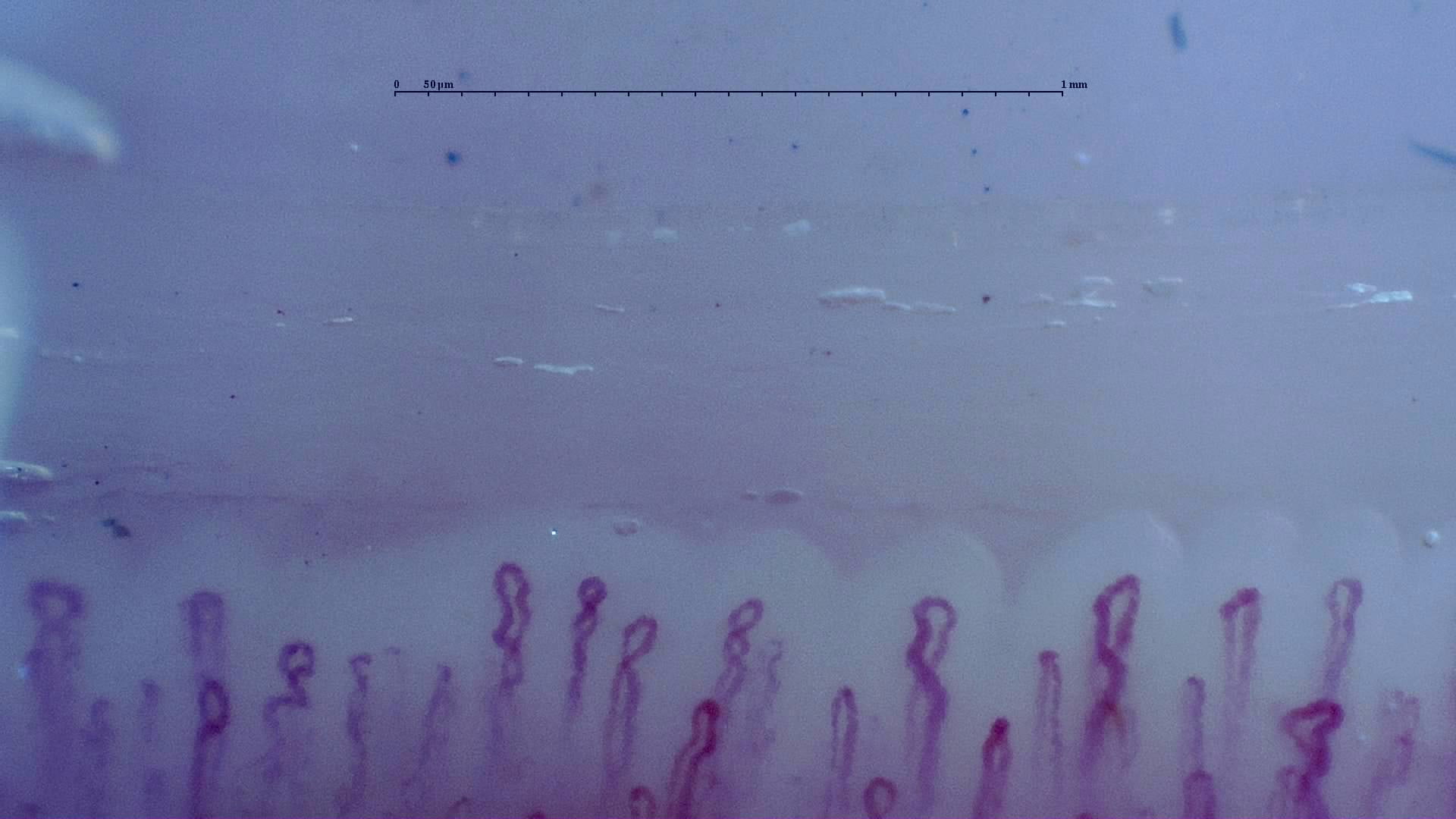
In clinical practice, simple tortuosity or a capillary with one or two crossings may still fit within normal variability, whereas repeated loss of apical convexity, marked homogeneous dilations, or extensive abnormal shapes should raise the level of suspicion [3, 5, 6].
Flow, background, and pericapillary area
Capillary flow, tissue background color, and visibility of the pericapillary halo may provide context, but today they are less standardized than density, diameter, or hemorrhages [1, 2]. They should therefore be described as complementary findings, not as the main axis of the conclusion. A pale or congestive background, for example, may depend on functional perfusion as much as on temperature, pressure, or skin transparency [1, 2].
Variability and confounders
Much overdiagnosis begins here: biological differences or acquisition artifacts are mistaken for true structural damage.
| Factor | How it may influence the study (usual findings) | What to do in practice |
|---|---|---|
| Skin phototype | Lower capillary visibility and lower quantified densities in studies of healthy adults [4] | Do not simply apply light-skin thresholds to every patient |
| Pediatric age | Density and measurements differ from adult values [7] | Avoid extrapolating adult criteria to children and adolescents |
| Fifth fingers | Lower mean density than other fingers [7] | Confirm borderline findings in several fingers, not only in little fingers |
| Local trauma, nail biting, or manicure | Hemorrhages and periungual distortion [1, 2, 8] | Record the exposure and avoid overreacting to isolated findings |
| Cardiovascular factors | Tortuosity, abnormal shapes, or lower density of low specificity [9, 10] | Integrate vascular context before inferring connective tissue disease |
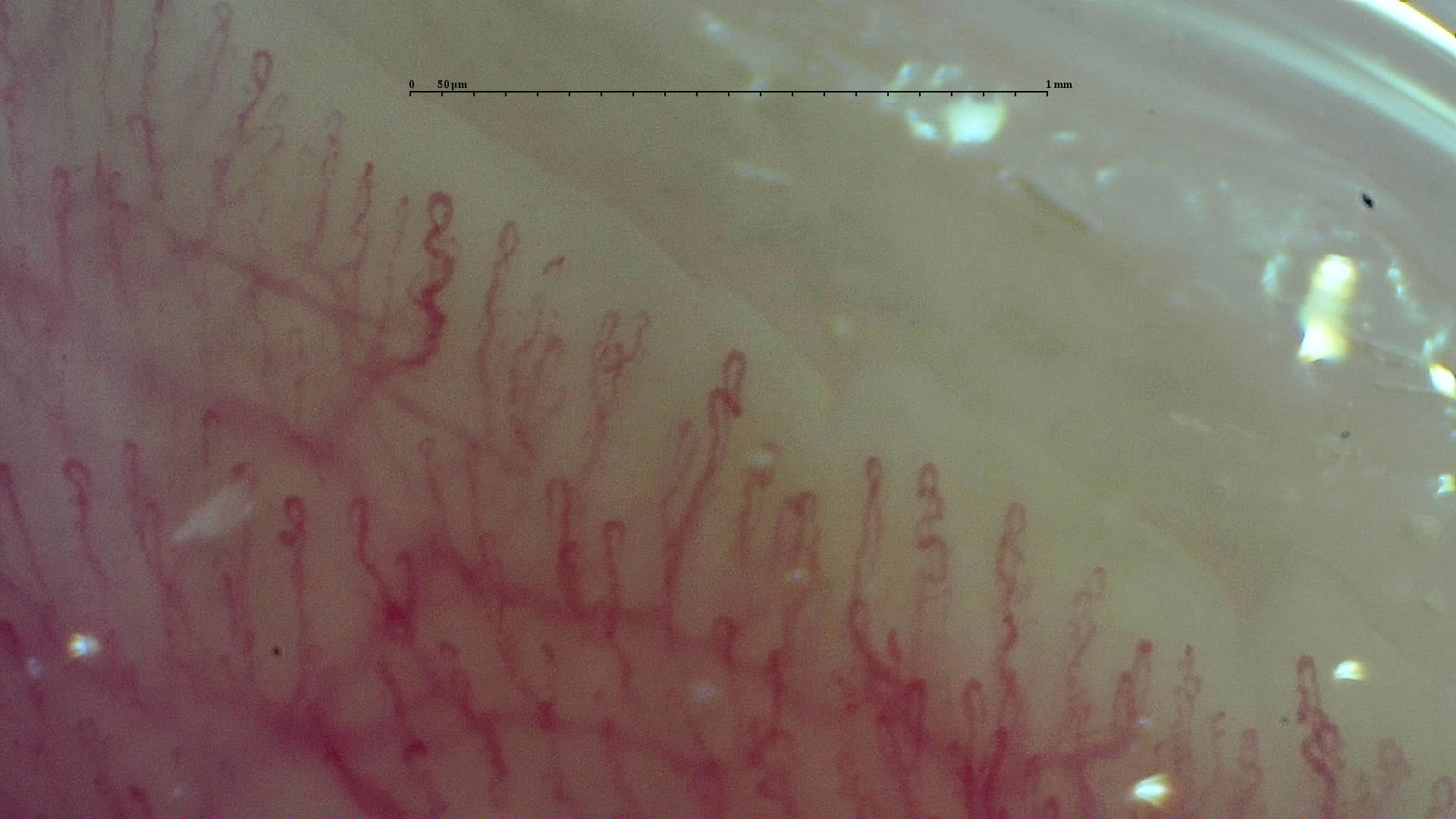
The effect of skin phototype is particularly important. In one quantitative study, median density progressively decreased from phototypes III to VI, reaching values clearly below classic ranges based on light-skin populations [4]. In an observational cohort of healthy individuals with phototypes III to V, tortuous, meandering, dilated capillaries and visible venous plexus were also frequent without implying connective tissue disease [11].
There is also noise outside rheumatology. A systematic review of non-rheumatic conditions and a 2024 study on cardiovascular risk factors show associations between capillaroscopic abnormalities and age, obesity, hypertension, alcohol, or smoking, mainly in relation to abnormal shapes, dilations, and hemorrhages [9, 10]. The practical consequence is simple: the more nonspecific the finding, the more important it is to interpret it according to pre-test probability.
Artifacts and gray zones
Between normal and pathological there is an intermediate zone of findings that require caution, repetition, or simply more honest wording.
Cosmetics, visible residues, and microtrauma
The traditional recommendation has been to avoid recent manicure and check for visible cosmetic residues before the examination. Recent literature, however, adds nuance: in a cohort of patients exposed to nail polish, acrylic nails, or henna, cosmetics generated artifacts and more nonspecific abnormalities, but removing nail polish ten days earlier did not clearly reduce abnormal findings [8]. In other words, cosmetics have an influence, but visible cosmetic residue does not automatically invalidate the study, and part of the problem may also depend on associated microtrauma [8].
How to handle "borderline" findings
| Situation | Cautious reading | What to do |
|---|---|---|
| Isolated tortuosity or one or two crossed capillaries | Compatible with a normal variant or nonspecific abnormality [3, 5, 6, 11] | Do not overdiagnose without other findings |
| Single hemorrhage | Assess local trauma, nail biting, or manicure [1, 2, 8] | Describe it, but do not turn it into a pattern |
| "Borderline" density with high phototype or poor transparency | Possible limitation due to poor visualization rather than true rarefaction [4, 11] | Repeat, review other fingers, and state the limitation |
| Visible venous plexus without other changes | Isolated low-specificity finding [11] | Report it as context, not as a defining lesion |
| Several mild abnormalities in a low-risk patient | Nonspecific rather than pathological pattern [1, 2, 3, 9, 10] | Integrate clinical context and consider follow-up if suspicion persists |
The following observation helps explain why these gray zones exist. In the EULAR group study, agreement for distinguishing normal from abnormal capillaries was moderate when all capillaries were analyzed, with kappa estimates around 0.40-0.47. However, it improved clearly when only capillaries considered classifiable were analyzed, with kappas between 0.62 and 0.81 [5]. This argues for more demanding practice: if a loop cannot be classified safely, it is better to declare it doubtful or non-evaluable than to assign it excessive meaning [5, 6].
Safe reading checklist
- Confirm that the first capillary row is visible and reasonably focused.
- Review several fingers before concluding that density is low or the pattern is abnormal [1, 2, 7].
- Contextualize skin phototype, pediatric age, local trauma, and recent cosmetics [4, 7, 8].
- Describe whether abnormalities are isolated, repeated, or combined [1, 2, 3].
- Do not use flow, background color, or visible venous plexus as the main isolated criterion [1, 2, 11].
- If clinical suspicion is low and the finding is mild, prefer the category of nonspecific abnormality over defined microangiopathy [1, 2, 3, 9, 10].
FAQ
Is there a single number of capillaries per millimeter that defines normality?
No. Classic ranges are useful as a starting point, but skin phototype, age, and the finger examined modify quantification. An isolated threshold is not enough by itself to define normality or disease [1, 2, 3, 4, 7].
Are tortuosities always pathological?
No. Mild tortuosities or one or two crossings may be seen in healthy people. Their prognostic value changes when they are very frequent, are combined with density loss, or appear within a coherent global pattern [3, 5, 6, 11].
Does an isolated hemorrhage require suspicion of connective tissue disease?
No. It may be due to microtrauma or cosmetics. It gains weight when it is repeated, recent, and coexists with dilations or rarefaction [1, 2, 3, 8].
Can a study with a mild variant still be called normal?
Yes, as long as the global pattern remains compatible with normality and the variants are scarce or nonspecific. "Normal with nonspecific variants" is also a valid conclusion [1, 2, 3, 6].
Is a visible venous plexus pathological?
Not necessarily. It may be observed in healthy individuals and has low specificity when it appears in isolation [11].
Do nail cosmetics always invalidate the study?
Not always. They may produce artifacts and should be documented, but recent evidence does not support the idea that removing nail polish several days beforehand completely eliminates nonspecific findings [8].
Should similar normality criteria be used in children and adults?
No. Pediatric populations have different distributions, and adult reference points should not simply be applied to them [7].
Glossary
- Normal pattern
- Study without a structural microangiopathy pattern, with preserved architecture and no coherent combination of giant capillaries, repeated hemorrhages, and rarefaction.
- Nonspecific abnormality
- Isolated or low-frequency finding that does not, by itself, allow attribution of a defined microangiopathy.
- Capillary density
- Number of visible distal capillary loops per linear millimeter in the nailfold distal row.
- Subpapillary venous plexus
- Superficial venous network that may become visible in some individuals without implying, by itself, specific pathology.
- Classifiable capillary
- Capillary loop with sufficient image quality for its shape to be described reproducibly.
References
- Smith V, Ickinger C, Hysa E, Snow M, Frech T, Sulli A, et al. Nailfold capillaroscopy. Best Pract Res Clin Rheumatol. 2023;37(1):101849. doi: 10.1016/j.berh.2023.101849. PMID: 37419757.
- Smith V, Herrick AL, Ingegnoli F, Damjanov N, De Angelis R, Denton CP, et al. Standardisation of nailfold capillaroscopy for the assessment of patients with Raynaud's phenomenon and systemic sclerosis. Autoimmun Rev. 2020;19(3):102458. doi: 10.1016/j.autrev.2020.102458. PMID: 31927087.
- Ingegnoli F, Gualtierotti R, Lubatti C, Bertolazzi C, Gutierrez M, Boracchi P, et al. Nailfold capillary patterns in healthy subjects: a real issue in capillaroscopy. Microvasc Res. 2013;90:90-95. doi: 10.1016/j.mvr.2013.07.001. PMID: 23880032.
- Bairwa D, Kavadichanda CG, Dunga S, Mathew A, et al. Effect of skin phototype on quantitative nailfold capillaroscopy. J Scleroderma Relat Disord. 2022;7(3):197-203. doi: 10.1177/23971983221102688. PMID: 36211202.
- Smith V, Beeckman S, Herrick AL, Decuman S, Deschepper E, De Keyser F, et al. An EULAR study group pilot study on reliability of simple capillaroscopic definitions to describe capillary morphology in rheumatic diseases. Rheumatology (Oxford). 2016;55(5):883-890. doi: 10.1093/rheumatology/kev441. PMID: 26843483.
- Cutolo M, Melsens K, Herrick AL, Foeldvari I, Leone MC, Mostmans Y, et al. Reliability of simple capillaroscopic definitions in describing capillary morphology in rheumatic diseases. Rheumatology (Oxford). 2018;57(4):757-759. doi: 10.1093/rheumatology/kex460. PMID: 29361155.
- Melsens K, Cutolo M, Schonenberg-Meinema D, Foeldvari I, Leone MC, Mostmans Y, et al. Standardized nailfold capillaroscopy in children with rheumatic diseases: a worldwide study. Rheumatology (Oxford). 2023;62(4):1605-1615. doi: 10.1093/rheumatology/keac487. PMID: 36005889.
- Shenavandeh S. Does the use of nail cosmetics interfere with the reporting of nailfold capillaroscopy? Clin Rheumatol. 2023;42(5):1307-1313. doi: 10.1007/s10067-023-06503-0. PMID: 36624179.
- Ciaffi J, Ajasllari N, Mancarella L, Brusi V, Meliconi R, Ursini F. Nailfold capillaroscopy in common non-rheumatic conditions: a systematic review and applications for clinical practice. Microvasc Res. 2020;131:104036. doi: 10.1016/j.mvr.2020.104036. PMID: 32603698.
- Álvarez Andrés E, de Miguel E, García de Yébenes MJ, Carmona L, Gómez Miranda C, Collado Ramos P, et al. Relationship between nailfold videocapillaroscopic findings and cardiovascular risk factors. Microvasc Res. 2024;154:104693. doi: 10.1016/j.mvr.2024.104693. PMID: 38701966.
- Gorasiya AR, Mehta HH, Prakashey A, Dave M. Nailfold Capillaroscopy of Healthy Individuals - An Observational Study. Indian Dermatol Online J. 2022;13(5):600-605. doi: 10.4103/idoj.idoj_80_22. PMID: 36304665.
- Hoerth C, Kundi M, Katzenschlager R, Hirschl M. Qualitative and quantitative assessment of nailfold capillaries by capillaroscopy in healthy volunteers. Vasa. 2012;41(1):19-26. doi: 10.1024/0301-1526/a000159. PMID: 22247056.