Capillaroscopy semiology and reporting
Interpreting a capillaroscopy is not a matter of listing striking findings, but of describing reproducibly what is seen, how reliably it was seen, and what it may mean in context. Capillaroscopic semiology requires standardized language, separation of isolated abnormalities from coherent patterns, and cautious conclusions [1, 2, 3, 7, 13].
- The observer's first obligation is to describe the image well before labeling it as "normal", "nonspecific", or "scleroderma pattern" [1, 2, 3].
- Density, dilation, giant capillaries, hemorrhages, abnormal shapes, and disorganization should be assessed systematically and in the distal row [1, 2, 3, 8].
- Isolated abnormalities may be nonspecific; interpretive weight increases when several abnormal domains converge into a reproducible pattern [1, 2, 4].
- A good report should include study quality, fingers assessed, surface area or sectors analyzed, described domains, a concise conclusion, and technical limitations when present [7, 8, 10, 13, 14].
- Reproducibility improves with simple definitions, structured training, and homogeneous quantification methods, not only with informal experience [3, 5, 6, 9].
Learning path
If you want to write more useful and consistent reports, this unit will help you separate description, interpretation, and diagnostic caution. It will be especially useful if you have already reviewed normality and variability, and you can then transfer this language to concrete clinical decisions in indications and clinical utility.
How to read an image
Before looking for giant capillaries or hemorrhages, always perform the following check: semiology starts by confirming that the image is interpretable and that the structure being examined is truly the distal capillary row.
First: quality and location
Interpretation should begin with three simple questions. Is visibility good, fair, or poor? Is the first capillary row identifiable? Is the image affected by pressure, reflections, cuticular trauma, or poor focus? This preliminary step, although it may seem procedural, prevents frequent errors such as calling a poorly centered area "capillary loss" or considering a traumatic hemorrhage pathological [1, 2, 8, 10].
A serious report can and should state, when appropriate, that part of the study is suboptimal. Technical caution is also clinical information. If the limitation is not acknowledged, the conclusion gains false certainty and loses value.
Then: move from the individual capillary to the global pattern
Useful reading is not limited to pointing out "pretty" or "odd" capillaries. It should integrate at least density, size, morphology, hemorrhages, and global architecture [1, 2, 3]. A single isolated finding may be nonspecific; several concordant findings repeated in different fingers carry much more interpretive weight.
| Reading question | What to look at | Common error |
|---|---|---|
| Is the image interpretable? | Visibility, focus, reflections, pressure | Starting measurements in a poor image |
| Is the distal row recognizable? | Loop alignment and anatomical orientation | Counting capillaries outside the useful row [1, 2, 8] |
| Are there isolated abnormalities or a pattern? | Consistency between fingers and affected domains | Overinterpreting a single abnormality [1, 4] |
| What is structural and what may be artifactual? | Trauma, manicure, skin phototype, edema, compression | Confusing traumatic fragility with microangiopathy |
Main semiological descriptors
Useful semiology needs few descriptors, but they must be well defined. The more ambiguous terms are introduced, the worse interobserver reproducibility usually becomes.
Capillary density
Density is the number of visible capillaries per linear millimeter in the distal row. In healthy adults, most series place practical normality around 7-10 capillaries per mm, although the exact value depends on method, device, and reference population [1, 2, 4, 6]. Clearly reduced density gains clinical meaning when accompanied by disorganization, dilations, or abnormal shapes, not when it appears as an isolated and doubtful finding.
Dilations and giant capillaries
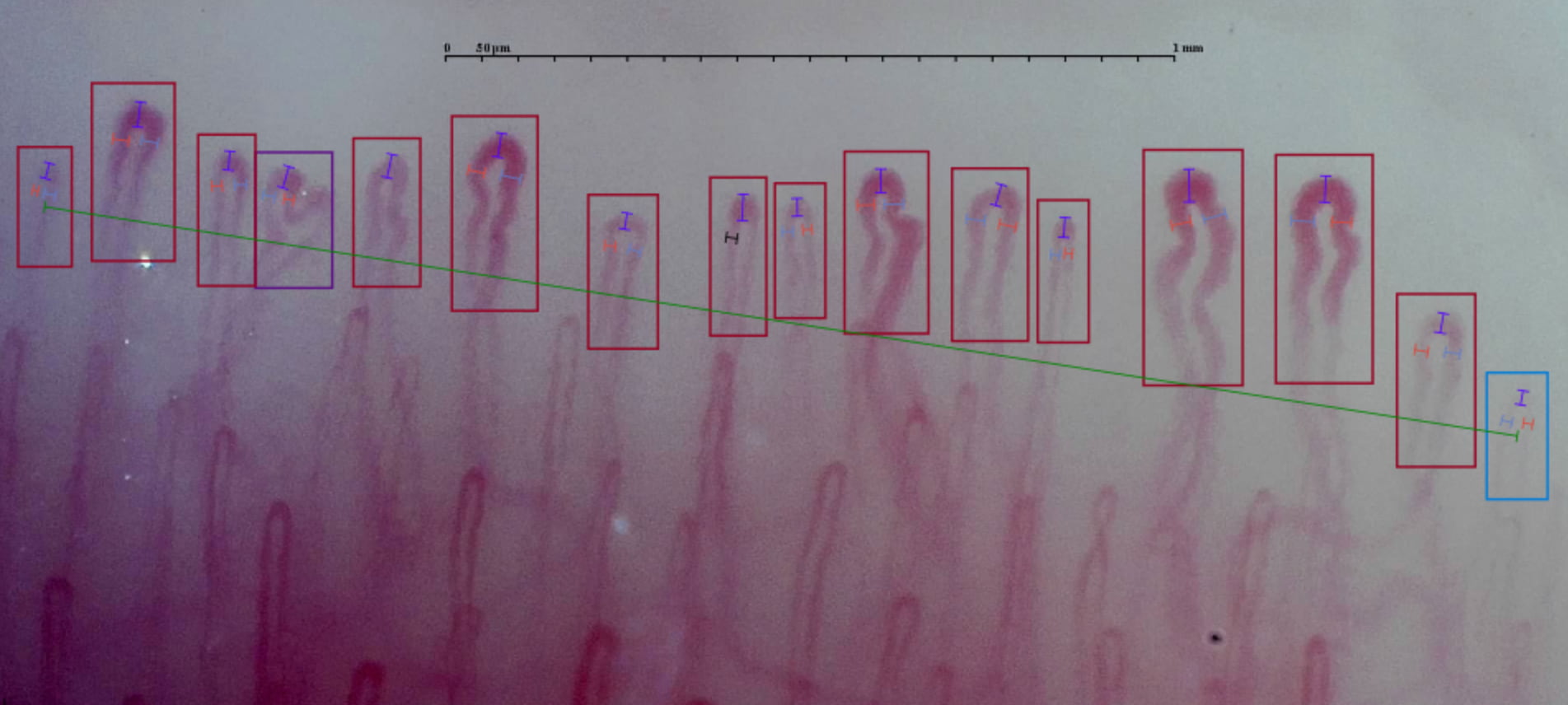
Size matters because progressive loop dilation is one of the most useful findings in scleroderma-pattern microangiopathy. Practically, many series and operational reviews describe loops with apical diameter >20 μm as dilated or ectatic and reserve the term giant capillary for homogeneously dilated loops reaching or exceeding 50 μm [11]. Even so, these thresholds should not be turned into dogma: more recent reviews remind us that normal apical width may lie approximately between 10 and 25 μm depending on method, calibration, and the population studied [12]. An isolated giant capillary is not enough to summarize an entire study, but it should not be ignored either, especially in patients with Raynaud's phenomenon [1, 2].
Language should also be harmonized. In these texts we prefer giant capillary and abnormal shapes, because recent reviews and definitions tend to use this vocabulary. If you review classic articles, you will still find megacapillary and ramified capillary or ramification; in most clinical contexts they describe the same domains, but with earlier nomenclature [1, 3, 11].

Morphology and architecture
Simple tortuous shapes, some "S" variations, and even certain isolated abnormalities may fall within the spectrum of normality or nonspecificity [3, 4]. Meaning changes when frankly abnormal capillaries, loss of apical convexity, complex abnormal shapes, or clear disorganization of the capillary bed appear. The literature addressing the reliability of simple definitions shows that it is preferable to use understandable and reproducible categories rather than an exuberant but inconsistent vocabulary [3].
Hemorrhages
Capillary hemorrhages represent blood extravasation and may be seen in isolation after microtrauma or cuticular manipulation. Their clinical interest increases when they are numerous, repeated, distributed in a way compatible with structural damage, and accompanied by other microangiopathic signs [1, 2, 8]. In other words, an isolated hemorrhage in a finger with a traumatized cuticle does not carry the same weight as several recent hemorrhages in a Raynaud context with dilations and density loss.

Abnormal shapes, neoangiogenesis, and disorganization
Complex abnormal shapes and neoangiogenesis are usually interpreted as markers of disordered vascular repair in more evolved microangiopathy, especially when combined with capillary rarefaction and loss of the usual architecture [1, 2]. This group still includes many images that were classically described mainly as ramified or bushy capillaries. Even here, absolutism should be avoided: one isolated abnormal shape may be nonspecific, whereas a set of bushy capillaries, disorganized architecture, and low density draws a much stronger pattern.
Pericapillary area, subpapillary plexus, and flow
These domains may provide context, but they are usually less robust than density, size, or hemorrhages. Pericapillary edema, striking visibility of the subpapillary plexus, or subjectively slowed flow may have descriptive interest, although they are vulnerable to technique, skin phototype, age, or skin thinning [1, 4, 8, 10]. They should therefore not be used as the main axis of the conclusion when the rest of the study is not coherent, or not unequivocally coherent, with an abnormal pattern.
| Domain | What to describe | What gives it more clinical weight | Common error |
|---|---|---|---|
| Density | Number of capillaries per mm and distribution | Repeated reduction in several fingers [1, 2, 6] | Counting outside the distal row |
| Dilation | Widened loops, apical or diffuse | Persistence and association with other abnormalities | Calling a doubtful measurement a giant capillary |
| Hemorrhages | Number, distribution, and appearance | Multiplicity and microangiopathy context [1, 8] | Not checking cuticle or local trauma |
| Morphology | Tortuosity, loss of convexity, abnormal shapes | Repeated abnormal capillaries and altered architecture [3] | Using different terms for the same lesion |
| Architecture | Palisade order or disorganization | Association with rarefaction and neoangiogenesis | Confusing technical deficiency with real disorganization |
From finding to report
The capillaroscopy report should not be a mere collection of adjectives. It should help the clinician understand what was seen, how reliable the observation was, and what it means, all without overstating the conclusion.
Minimum useful structure
The set of minimum domains proposed in 2024 for capillaroscopy reporting supports a very practical idea: the report should include basic study conditions, fingers assessed, quality or visibility, structured findings, and a final conclusion [7]. A 2026 Italian study using Delphi methodology concretized this logic into a 23-item checklist, 16 of them mandatory, distributed across general aspects, examined fingers, confounding factors, device description, image quality, and examination details [13]. In clinical practice, this workflow can become a short but consistent template.
The report should also make clear what coverage the study actually had. In the multicenter study by Guillén del Castillo et al., using 16 medial images instead of 32 images with medial and lateral fields changed pattern assignment in a relevant proportion of cases, including changes between systemic sclerosis pattern and non-systemic sclerosis pattern [14]. Therefore, "eight fingers examined" is less informative than specifying number of images, sectors, and coverage limitations.
| Report block | What should be included | Brief example |
|---|---|---|
| Study conditions | Number of fingers, global quality, technical limitations | "Eight fingers examined; good visibility except left fourth finger due to trauma" |
| Capture coverage | Number of images, medial/lateral fields, and approximate length analyzed | "32 images; four fields per finger in eight non-thumb fingers" |
| Structured description | Density, dilation, hemorrhages, morphology, architecture | "Preserved density; no giant capillaries; isolated traumatic hemorrhages" |
| Interpretive synthesis | Normal, nonspecific, or pattern compatible with microangiopathy | "Study without scleroderma pattern" |
| Cautious observation(s) | Limitations or need for follow-up | "If clinical suspicion persists, consider longitudinal repeat examination" |
One fundamental principle makes the written report truly useful: description must be separated from interpretation. In other words, conclusions should not go beyond the image. For example, it is more precise to write "findings compatible with a scleroderma pattern" than to assert a complete diagnosis of connective tissue disease without integrating clinical assessment and serology.
Example of a short and useful report
Study quality: good. Eight evaluable fingers; left second finger with fair visibility due to manipulated cuticle.
Findings: globally preserved density, no giant capillaries or avascular areas. Two focal hemorrhages in the left second finger, probably related to local trauma. Preserved palisade architecture.
Conclusion: study without scleroderma pattern. Focal nonspecific traumatic abnormalities. Correlate clinically; repeat if high suspicion persists.
Conclusions to avoid
- Diagnosing connective tissue disease from the image alone.
- Calling a single poorly documented isolated abnormality a "scleroderma pattern".
- Confusing poor technical quality with pathological findings.
- When relevant, omitting the limitation that not all fingers could be adequately assessed.
Quantification, reproducibility, and scores
Quantification improves comparability, but only when it starts from stable definitions and well-acquired images. In semiology, it is better to describe well than to measure badly.
Why reproducibility matters
The literature on procedural reliability shows that observer agreement improves when simple definitions and structured training are used. A pilot study by the European Alliance of Associations for Rheumatology (EULAR) group suggested that identification of several morphological traits reaches moderate-to-good agreement when standardized definitions are used as a reference [3]. In addition, reproducibility of the scleroderma pattern improves when reading is performed with wide-field images and shared criteria [5].
A recent trial added another important point: an online course with a support algorithm improved capillaroscopy interpretation among observers with different levels of experience [9]. The message is useful for any department aiming to implement the technique: training the team in language and process may be as beneficial as buying a new device.
When to quantify
Quantification makes sense when visits will be compared, microvascular damage will be stratified, or interpretive variability needs to be reduced. The most feasible routine variables are usually density, number of giant capillaries, hemorrhages, and some linear parameters, always with homogeneous methodology [1, 6]. In daily practice, exhaustive quantification of every morphological finding takes time and does not always add value in the same proportion.
That limit changes when quantification stops being manual. With artificial intelligence (AI) tools and automated analysis, exhaustive measurement can be immediate, reproducible, and easy to integrate into the report; in that scenario, there is no practical reason to give up objectively documenting more information, provided the image is adequate and the method is controlled. Platforms such as Capillary.io allow studies with multiple images to be organized, capillaries to be detected and measured, quantitative variables to be summarized, quality to be assessed, and standardized reports to be generated with much lower operational burden [15]. To go deeper into this approach, review the unit on AI, quantification, and reproducibility in capillaroscopy.
What role do scores play?
Semiquantitative and quantitative scales exist to describe microvascular damage, especially in systemic sclerosis. Their utility is greater in structured follow-up or research than in isolated routine examinations [1, 6]. The practical point is not to make the score an end in itself. A bare number obtained without acquisition quality or clinical context may look precise, but it does not provide true validity.
| Abnormality | Definition | Score* |
|---|---|---|
| Giant capillaries | Loops with apical diameter ≥ 50 μm | 0-3 |
| Hemorrhages | Microhemorrhages or pericapillary hemosiderin deposits | 0-3 |
| Capillary loss | Reduced number of loops with avascular areas | 0-3 |
| Disorganization | Loss of the usual parallel architecture of the capillary bed | 0-3 |
*Scoring criteria: 0, absent; 1, <33% of the field; 2, 33-66% of the field; 3, >66% of the field.
Short clinical cases and common errors
Short examples help fix judgment. Most interpretive failures do not come from not knowing a definition, but from applying it outside context.
Case 1: isolated tortuosity in a healthy patient
A 34-year-old woman without Raynaud or known autoimmunity. Some simple sinuous capillaries are seen, with preserved global architecture. The cautious conclusion is not "pathological", but findings within the nonspecific spectrum or the broader range of normality [3, 4]. The error would be to attribute disproportionate meaning to them simply because they are visually striking.
Case 2: hemorrhages after manicure
Patient with mild Raynaud and recent manicure. Multiple small focal hemorrhages in two fingers, without dilations or density loss. In this situation, semiology must separate the finding from its interpretation: focal hemorrhages probably traumatic; study not conclusive for structural microangiopathy; consider repeating.
Case 3: a truly concerning pattern
Patient with Raynaud. Repeated giant capillaries, hemorrhages, and reduced density are observed in several fingers. Positive antinuclear antibodies (ANA) and puffy fingers are also documented. Here, value lies not in a single descriptor but in the convergence of several abnormal domains. The report should describe them separately and conclude that there is a pattern compatible with scleroderma-pattern microangiopathy, while avoiding an isolated clinical diagnosis.
Real cases
Practice with complete capillaroscopy studies
Review real clinical cases with context, images, quantified findings, and an interactive viewer to train semiological reading in specific clinical situations.
View real clinical casesFAQ
What carries more weight: an isolated finding or the global pattern?
In general, the global pattern. An isolated finding may be nonspecific; several coherent abnormal domains have greater interpretive value [1, 2, 4].
Does an isolated hemorrhage require suspicion of connective tissue disease?
No. Local trauma, manicure, and clinical context should be reviewed before attributing microangiopathic significance to it [1, 8].
When can I call something a giant capillary?
Most consensuses and reviews place the practical threshold at 50 μm or more, provided measurement is reliable and the image is well calibrated. Below this point, many series describe dilation from >20 μm, although normal apical width may approach ~25 μm in some contexts [11, 12].
Should flow be described in every report?
It may be added as an observation, but it is usually less robust than density, size, or hemorrhages, and it should not be the main support for the conclusion [1, 8, 10].
Can I conclude "systemic sclerosis" from capillaroscopy?
Not in isolation. The correct approach is to describe a pattern compatible with scleroderma-pattern microangiopathy and integrate it with clinical assessment and serology [1, 2, 7].
Glossary
- Capillary density
- Number of visible capillaries per linear millimeter in the distal row analyzed.
- Giant capillary
- Homogeneously dilated capillary loop; it is the preferred term in many recent texts and corresponds to the historical megacapillary. When measurement is reliable, it is usually reserved for 50 μm or more; below that point, many series describe dilation (without calling it giant) from >20 μm.
- Abnormal shape
- Umbrella term for irregular capillary morphologies; in classic literature it often overlaps with ramified capillaries or ramifications.
- Disorganization
- Loss of regular palisade architecture with heterogeneous orientation and distribution.
- Structured report
- Report that separately considers study conditions, findings, conclusion, and uncertainties or limitations.
- Reproducibility
- Ability of different observers, or the same observer at another time, to reach comparable conclusions from the same material.
References
- Smith V, Ickinger C, Hysa E, Snow M, Frech T, Sulli A, et al. Nailfold capillaroscopy. Best Pract Res Clin Rheumatol. 2023;37(1):101849. doi: 10.1016/j.berh.2023.101849. PMID: 37419757.
- Smith V, Herrick AL, Ingegnoli F, Damjanov N, De Angelis R, Denton CP, et al. Standardisation of nailfold capillaroscopy for the assessment of patients with Raynaud's phenomenon and systemic sclerosis. Autoimmun Rev. 2020;19(3):102458. doi: 10.1016/j.autrev.2020.102458. PMID: 31927087.
- Smith V, Beeckman S, Herrick AL, Decuman S, Deschepper E, De Keyser F, et al. An EULAR study group pilot study on reliability of simple capillaroscopic definitions to describe capillary morphology in rheumatic diseases. Rheumatology (Oxford). 2016;55(5):883-890. doi: 10.1093/rheumatology/kev441. PMID: 26843483.
- Ingegnoli F, Gualtierotti R, Lubatti C, Bertolazzi C, Gutierrez M, Boracchi P, et al. Nailfold capillary patterns in healthy subjects: a real issue in capillaroscopy. Microvasc Res. 2013;90:90-95. doi: 10.1016/j.mvr.2013.07.001. PMID: 23880032.
- Boulon C, Blaise S, Lazareth I, Le Hello C, Pistorius MA, Imbert B, Mangin M, Sintes P, Senet P, Decamps-Le Chevoir J, Tribout L, Carpentier P, Constans J. Reproducibility of the scleroderma pattern assessed by wide-field capillaroscopy in subjects suffering from Raynaud's phenomenon. Rheumatology (Oxford). 2017 Oct 1;56(10):1780-1783. doi: 10.1093/rheumatology/kex282. PMID: 28957564.
- Herrick AL, Berks M, Taylor CJ. Quantitative nailfold capillaroscopy-update and possible next steps. Rheumatology (Oxford). 2021;60(5):2054-2065. doi: 10.1093/rheumatology/keab006. PMID: 33493310.
- El Miedany Y, Ismail S, Wadie M, Müller-Ladner U, Giacomelli R, Liakouli V, et al. Development of a core domain set for nailfold capillaroscopy reporting. Reumatol Clin (Engl Ed). 2024;20(7):345-352. doi: 10.1016/j.reumae.2024.07.003. PMID: 39160005.
- Karbalaie A, Emrani Z, Fatemi A, Etehadtavakol M, Erlandsson BE. Practical issues in assessing nailfold capillaroscopic images: a summary. Clin Rheumatol. 2019;38(9):2343-2354. doi: 10.1007/s10067-019-04644-9. PMID: 31278512.
- Ng SA, Tan WH, Saffari SE, Low AHL. Evaluation of Nailfold Capillaroscopy Online Training Using the Fast Track Algorithm. J Rheumatol. 2023;50(3):368-372. doi: 10.3899/jrheum.220794. PMID: 36455942.
- El Miedany Y, Ismail S, Wadie M, Hassan M. Nailfold capillaroscopy: tips and challenges. Clin Rheumatol. 2022;41(12):3629-3640. doi: 10.1007/s10067-022-06354-1. PMID: 36040673.
- Kubo S, Tanaka Y. Usefulness of nailfold videocapillaroscopy for systemic sclerosis. Inflamm Regen. 2016;36:5. doi: 10.1186/s41232-016-0001-x. PMID: 29259678.
- Herrick AL, Dinsdale G, Murray A. New perspectives in the imaging of Raynaud's phenomenon. Eur J Rheumatol. 2020;7(Suppl 3):S212-S221. doi: 10.5152/eurjrheum.2020.19124. PMID: 33164735.
- Ingegnoli F, Pireddu D, Platania E, De Angelis R, Alunno A, Ariani A, et al. Clinical practice guidelines for reporting nail fold videocapillaroscopy: a Delphi consensus on behalf of the Italian Society of Rheumatology study group on capillaroscopy. Clin Exp Rheumatol. 2026 Jan 15. doi: 10.55563/clinexprheumatol/2z4j95. Online ahead of print. PMID: 41537537.
- Guillén Del Castillo A, Lledó-Ibáñez GM, Sáez Comet L, Freire Dapena M, Mesa Navas M, Martín Cascón M, et al. Value of nailfold capillaroscopy in the classification of the systemic sclerosis pattern. Med Clin (Barc). 2026;166(6):107426. doi: 10.1016/j.medcli.2026.107426. PMID: 42013567.
- Capillary.io. Capillary.io features. Capillary.io; accessed July 3, 2026. Available at: https://es.capillary.io/funcionalidades/