Artificial intelligence, quantification, and reproducibility in capillaroscopy
AI is now inseparable from capillaroscopy. In 2024-2026, quantitative algorithms and machine-learning models have emerged that can classify patterns, detect structural abnormalities, and reduce part of the variability between observers; even so, their real usefulness depends more on labeling quality, quality assessment, external validation, the number of fingers and fields acquired, and standardization of reporting than on the raw number of parameters or the complexity of the model [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 24].
- Quantification does not replace semiological description; it organizes it. The most useful algorithms translate density, size, hemorrhages, and morphology into reproducible variables that are then interpreted clinically [1, 2, 3, 8, 9].
- The main problem these tools try to solve is not the lack of images, but interobserver subjectivity, especially when distinguishing normal from nonspecific patterns and when grading scleroderma patterns [3, 4, 5, 8, 9].
- In a standard nailfold videocapillaroscopy (NVC) protocol, one case may generate 32 images, with four fields per finger across eight fingers; rapid analysis and quality control are therefore no longer a "luxury" but a practical requirement [22, 24].
- Quality assessment is the most important filter in the AI workflow: if an image enters out of focus, poorly magnified, or poorly positioned, the classifier learns and decides on noise [2, 7, 11, 12, 13].
- Fast Track and CAPI-Score algorithms, together with the capillaroscopist's experience, remain the practical reference: automated models should be compared with well-trained observers, not with improvised readings [3, 5].
- CAPI-Score and CAPI-Detect represent two different strategies: CAPI-Score is based on simple rules derived from quantitative variables that can also be counted manually, whereas CAPI-Detect uses machine learning, incorporates more variables, and shows better discriminative ability when there is a high level of expert agreement [8, 9].
- External validation is more important than internal metrics. A model with a high area under the curve (AUC) or high accuracy can still lose value if the device, population, image quality, or reference standard changes [7, 8, 9, 10, 14].
- According to recent consensus documents, AI is clinically useful only if it is contextualized with standardized acquisition, quality control, potential confounders, and a structured report [2, 11, 12, 13].
Learning path
If you want to understand when quantification and AI really add value, this unit reviews their most relevant uses, limits, and biases. It will be especially useful if you already master acquisition and quality and semiological reading and reporting, because no algorithm can compensate for a poorly acquired image or weak clinical interpretation [1, 2, 3, 11, 12].
Why Quantify
Quantification was born from a concrete problem: two competent observers may easily agree on a clearly scleroderma pattern, but not always on a borderline image, a poor-quality study, or the distinction between normal and nonspecific [3, 4, 5].
The Fast Track algorithm from the European Alliance of Associations for Rheumatology (EULAR) already summarized part of this need with a simple decision tree to differentiate a scleroderma pattern from a non-scleroderma pattern, achieving very high kappa agreement estimates even among participants with varying levels of experience [3]. This reinforces a practical idea: before reaching AI, capillaroscopy had already shown that simplifying rules and harmonizing definitions improves reproducibility.
The reproducibility problem is not solved only with more informal training. A multicenter study by Dinsdale et al. showed that intra- and interobserver reliability for variables such as density, apical width, giant capillaries, or severity grade, although reasonable, is not perfect, even among experts [4]. Training also works better for some tasks than for others: in online Fast Track training, identification of scleroderma versus non-scleroderma pattern reached a mean interobserver kappa of 0.86, whereas differentiating normal from nonspecific did not exceed 0.59 [5].
Quantification therefore has two different aims. One is descriptive: to better measure density, size, or hemorrhages. The other is classificatory: to convert those measurements into a decision or probability. Caution is needed regarding the ability of AI to achieve this second aim, and it should not be treated as infallible [1, 2, 3, 4, 5, 8, 9].
What Is Being Measured Today
Current models no longer simply count capillaries. The trend is to convert the complete architecture of the distal bed into a set of continuous and reproducible variables [6, 7, 8, 9, 10].
In the most recent studies, quantified domains include capillary density per millimeter, percentage of giant capillaries, percentage of abnormal capillaries, tortuosity, hemorrhages, loop size, global shape, abnormal forms, and aggregate architectural variables [6, 7, 8, 9, 10]. Following a sequential-rule logic, CAPI-Score used thresholds for density, percentage of giant and abnormal capillaries, tortuosities, and hemorrhages [8]. CAPI-Detect broadened the spectrum and used 24 automatically extracted variables related to capillary architecture to train a CatBoost model [9].
This evolution matters because it changes the nature of the data. When a variable is measured continuously, it depends less on the observer's subjective language and becomes more comparable between centers, provided acquisition, quality control, and software are consistent [2, 6, 7, 8, 9, 11, 12, 13]. Even so, as a methodological inference, these systems learn from human consensus labels rather than from an independent biological gold standard [8, 9, 10].

| Domain | What it tries to objectify | Potential value | Common limitation |
|---|---|---|---|
| Density | Number of capillaries per mm in the distal row | Basis for classification and follow-up [2, 8, 9] | Depends on which segment and how many millimeters are analyzed |
| Size | Dilations and giants as continuous variables | Reduces subjectivity when calling a "giant capillary" [6, 7, 8, 9] | Requires calibration and good resolution |
| Abnormal capillaries | Loops with morphology outside the expected range | Helps differentiate patterns and severity [8, 9] | The exact definition may vary between software systems |
| Hemorrhages | Visible extravasations and their distribution | Add weight to classification [7, 8] | Highly sensitive to trauma and local confounders |
| Global architecture | Order, disorganization, abnormal forms, and combined density | Enables more complete ML models [9, 10] | Black-box risk if variables are not explained |
ML, machine learning.
Current Algorithms and Performance
Recent literature allows at least four levels of complexity to be distinguished: simplified clinical rules, automated quantification of discrete phenomena, quantitative rule algorithms, and more flexible machine learning [3, 6, 7, 8, 9, 10].
Fast Track as the baseline
Fast Track is not AI, but it remains the tool that makes the most sense clinically. Its value lies in offering a simple and highly reproducible rule to separate a scleroderma pattern from a non-scleroderma pattern, with mean Cohen's kappa (two observers) of 0.94 to 0.96 and Light's kappa (more than two observers) of 0.87 to 0.92 in EULAR and EUSTAR validations [3]. Many later developments, including CAPI-Score, are explicitly inspired by this logic [8].
Automated detection and external validation
Before classifying complete patterns, several groups addressed simpler tasks: detecting capillaries, measuring their size, and recognizing hemorrhages. In the series by Gracia-Tello BG et al., the performance metrics of the initial classification proposal reached a precision of 83.84% and a recall of 92.44% for identifying capillaries, with more modest performance when it had to classify specific shapes or sizes [6]. The subsequent external validation was more clinically relevant: with consensus from at least three experts, the software correctly predicted 75.8% of images; with consensus from at least four experts, agreement with the software rose to 87.1%, and the positive predictive value exceeded 80% for hemorrhages and for unaltered, giant, or abnormal capillaries [7].
CAPI-Score
CAPI-Score represents the step from simple detection to structured quantitative classification. Based on 851 capillaroscopies and 21,957 images agreed on by nine capillaroscopists, the algorithm established four rules. The first, to differentiate scleroderma from non-scleroderma pattern, reached an accuracy of 0.88; this reached 0.82 for the rules separating early, active, and late patterns; and for distinguishing normal from nonspecific pattern it was 0.73 [8]. The practical reading is clear: automation works better when the question is binary and clinically robust than when it is forced to distinguish neighboring and poorly defined categories.
CAPI-Detect and other machine-learning models
CAPI-Detect expanded the CAPI-Score strategy with 24 architectural variables and a machine-learning model. In 1,780 capillaroscopies blindly analyzed by three or four observers, when partial consensus existed between them, the model reached accuracies of 0.912, 0.812, and 0.746 for, respectively, distinguishing systemic sclerosis (SSc) from non-SSc, classifying scleroderma subpatterns, and differentiating normal from nonspecific pattern; when the analysis was limited to images with full consensus, accuracy rose to 0.910, 0.925, and 0.933 [9]. The improvement over CAPI-Score suggests that there is relevant morphological information that simplified manual rules do not fully capture.
Other AI approaches confirm the trend, but also its limits. Although the vision-transformer model by Garaiman A et al. obtained AUCs between 81.8% and 84.5% for microangiopathic signs and scleroderma pattern, trained rheumatologists still outperformed it on average [10]. And although a recent study exploring classification within systemic sclerosis documented accuracies above 98%, multicenter clinical validation is still needed to confirm the usefulness of this undoubtedly promising proposal [15].

| Tool / approach | What it solves | Published performance | Practical reading |
|---|---|---|---|
| Fast Track [3] | Simple manual classification, SSc vs non-SSc | Mean kappa 0.94-0.96; Light's kappa 0.87-0.92 | Still the clinical reference for simplicity and reliability |
| Initial automated pipeline [6] | Detection and classification of capillaries/hemorrhages | Precision 83.84%; recall 92.44% for capillary identification | Useful as a preceding step, not as an autonomous final report |
| External validation [7] | Reproducibility in images from different centers | 75.8% correct with expert consensus ≥3; 87.1% with consensus ≥4 | Validation outside the development center changes confidence substantially |
| CAPI-Score [8] | Classification by quantitative rules | Accuracy 0.88; 0.82; 0.73 depending on task | Very useful for well-defined tasks; weaker for normal vs. nonspecific |
| CAPI-Detect [9] | ML classification with 24 variables | Accuracy 0.912 / 0.812 / 0.746; up to 0.933 with full consensus | Promising, but highly dependent on labeling quality |
| Vision transformer [10] | Recognition of microangiopathic changes | AUC 81.8%-84.5% | Can help, but does not replace the trained expert |
ML, machine learning; SSc, systemic sclerosis.
Quality Assessment and Automated Feedback
The most unfairly neglected step in the AI workflow is not classification, but deciding whether the image deserves to be analyzed. In capillaroscopy, an invalid image is not simply "worse"; it can push the algorithm and the clinician toward an erroneous category [2, 11, 12, 13].
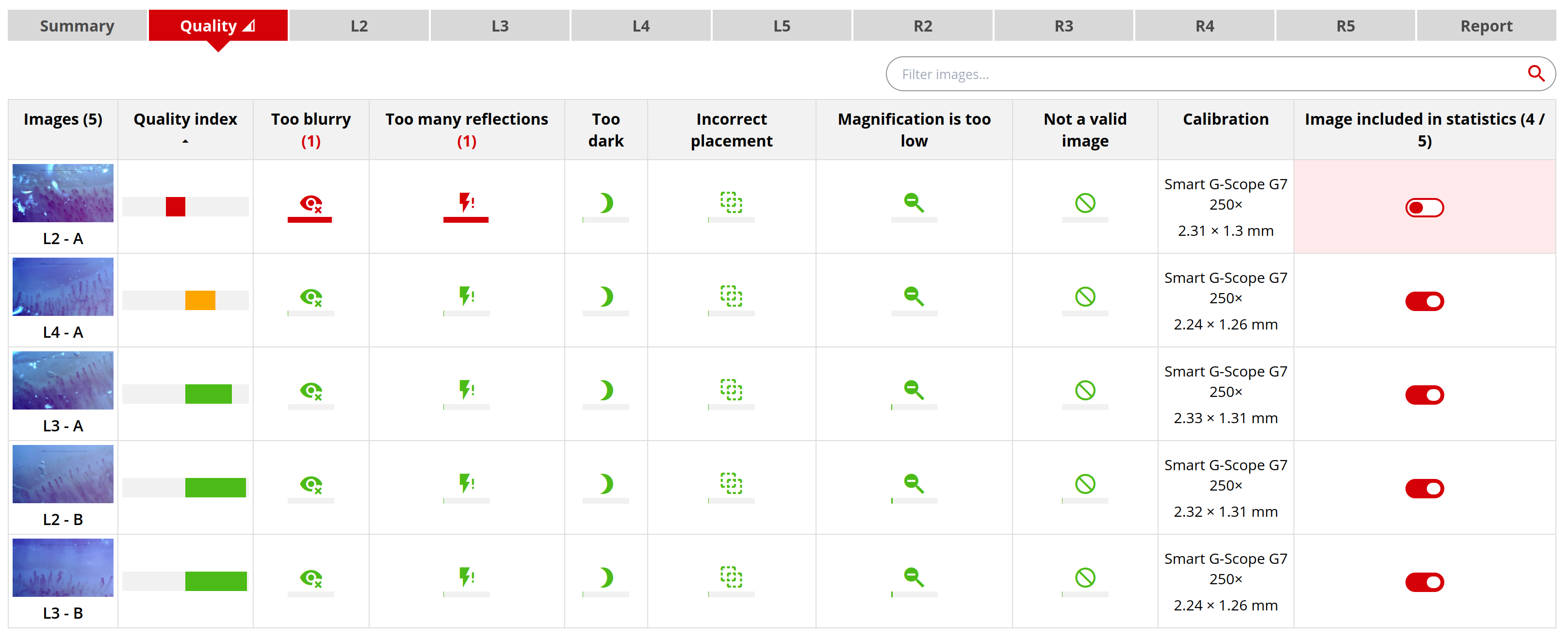
An ACR Convergence 2025 abstract from the American College of Rheumatology on Automated Feedback and Quality Control is especially useful in this context. It describes a system developed with a ConvNeXt V2 architecture and trained on 10,866 annotated images, capable of identifying common acquisition problems such as low magnification, poor focus, reflections, incorrect positioning, underexposure, and invalid content; for valid images, it also differentiates low from acceptable quality [13]. Reported performance was especially high for identifying (and therefore excluding the image in question, or interpreting it with caution in the final scenario): low magnification (F1-score 0.99); invalid content (F1 0.96); poor focus (F1 0.84); reflections (F1 0.83); low quality among valid images (F1 0.83) [13].
This finding is relevant. A good AI workflow in capillaroscopy should function as a four-link chain. First, acquisition. Second, quality assessment to exclude invalid images and provide immediate feedback to the operator. Third, quantification or classification only on acceptable images. Fourth, human review and report generation. If the second step is omitted, the rest of the process is exposed to the classic problem of garbage in, garbage out [2, 7, 11, 12, 13].
The impact of this second step is easier to understand when the real workload is considered. In a 2026 multicenter study focused on identifying systemic sclerosis patterns, the reference examination included 32 images per case, corresponding to four fields per finger in eight non-thumb fingers [24]. When a platform can analyze the quality of each image and immediately produce a quantitative summary of the capillaroscopy study, the benefit is not limited to saving the clinician minutes, for example by avoiding manual review of full batches of defective images; very importantly, it also allows the capture to be repeated during the same clinical encounter [13, 22, 24].
The value of quality assessment is not only technical. It is also educational. A system that detects insufficient magnification, reflections, or poor positioning in real time can accelerate the learning process for residents or young researchers and harmonize capture in multicenter studies, where the main source of variation is often not the final observer but how the images were obtained [7, 11, 12, 13].

| Quality problem | Clinical or algorithmic risk | Why it should be detected first |
|---|---|---|
| Low magnification | Underestimates morphological detail and biases classification | Avoids analyzing an image unable to show the distal row clearly [13] |
| Poor focus or reflections | Distorts borders, diameters, and hemorrhages | Reduces quantification and automated detection errors [7, 13] |
| Incorrect positioning | Considers structures outside the useful area | Prevents a mere framing problem from being called rarefaction [2, 11, 13] |
| Invalid content | Introduces noise into the model | The clearest example of an image that should be excluded [13] |
| Valid but low-quality image | Can be used, but with lower confidence | Allows deciding whether to repeat it or interpret it cautiously |
Capillary.io and published lines of work
Among platforms with visible scientific output, Capillary.io deserves attention because it allows one methodological line to be followed from initial automated detection to more complex classification models, sampling requirements, and more recently explicit quality assessment tools [6, 7, 8, 9, 13, 19, 20, 24].
According to the Capillary.io publications page, the sequence of publications associated with the platform includes initial work on automated detection and classification of capillaries and hemorrhages [6], external clinical validation of the software to identify structural abnormalities and hemorrhages [7], the CAPI-Score algorithm [8], the CAPI-Detect machine-learning model [9], the study of minimum sampling requirements to classify systemic sclerosis pattern [24], and the most recent contribution on automated feedback and real-time quality control [13, 19]. This set of contributions is useful because it is not a single isolated publication, but a development chain that allows methodological progression to be assessed.
Analysis of these contributions invites reflection. On one hand, editorial continuity helps show how a platform matures: first it detects, then validates, then classifies with rules, finally learns with more complex variables and also tries to control input quality before classification [6, 7, 8, 9, 13]. On the other hand, the fact that the same line of work generates several publications does not remove the need for independent validation, comparison with other approaches, and demonstration, if ultimately achieved, of clinical utility added to expert observation [7, 8, 9, 10].
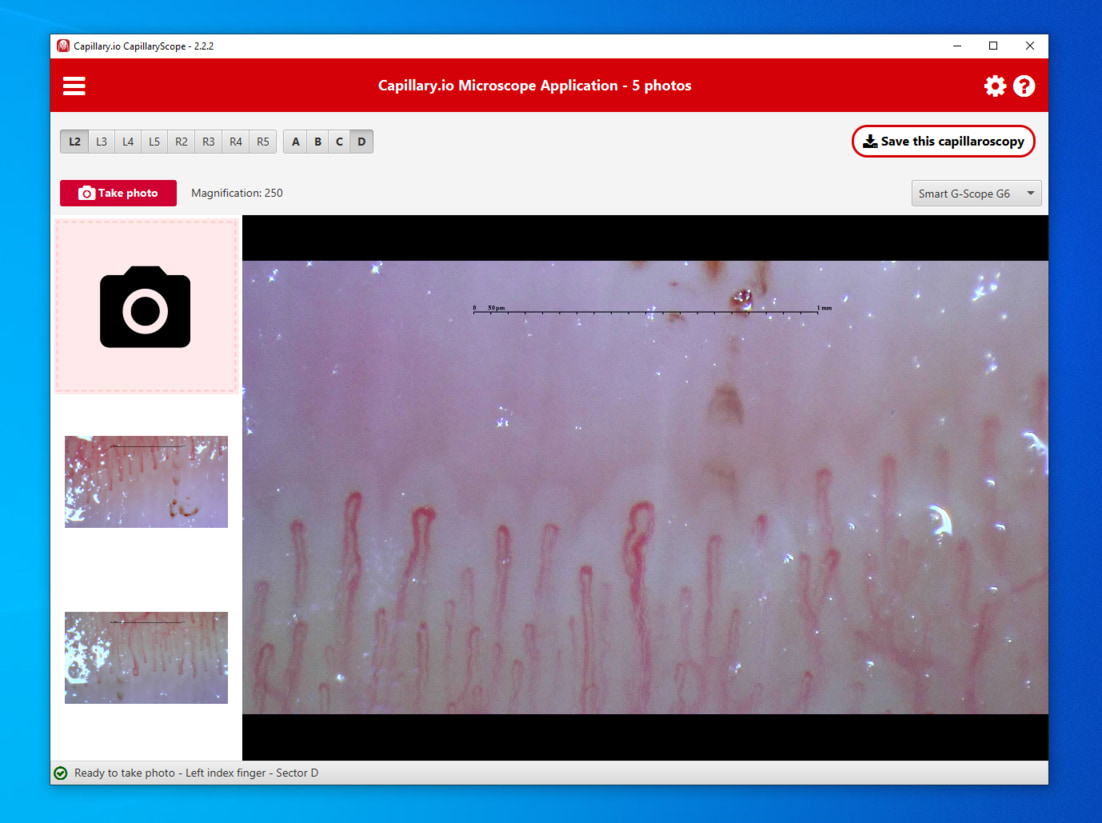
Guided capture from an app or local device allows calibration, image ordering, and transfer to the platform before quantitative analysis.
Capillary.io is also appearing in uses beyond classical systemic sclerosis. Another contribution presented at the same ACR 2025 meeting described the use of quantitative variables extracted by the platform to try to discriminate primary Raynaud's phenomenon from autoimmune diseases within the broad "drawer" of nonspecific patterns. The global F1-score was 0.632. Although performance was modest, the study is valuable because it confirms that the real challenge lies less in "clear" patterns than in the grey zone where clinical uncertainty is greatest [14]. In parallel, the multicenter CapIAMI project has already presented preliminary data in 272 patients with inflammatory myopathies, where the combination of automated capillaroscopic metrics and laboratory biomarkers reached an accuracy of 0.746 for predicting clinical activity [15, 20].
Expansion continues toward more descriptive scenarios and into pediatrics. Another study presented at ACR 2025 processed, with Capillary.io, a cohort of 136 autoimmune rheumatic diseases to describe capillaroscopic "signatures" in systemic sclerosis, polyautoimmunity, and pulmonary arterial hypertension [16]. Also in 2025, a juvenile dermatomyositis study used automated quantification of density and diameters to relate disease activity to lower density and larger loop caliber [17]. A previous pediatric study showed that automated quantification using a convolutional neural network (CNN) can cluster patients with juvenile dermatomyositis according to capillary morphology and myositis-specific autoantibody positivity [18]. Taken together, these contributions do not prove that the platform is "validated for everything"; rather, they show how automation is beginning to move beyond the scleroderma niche and explore new phenotypes [14, 15, 16, 17, 18].
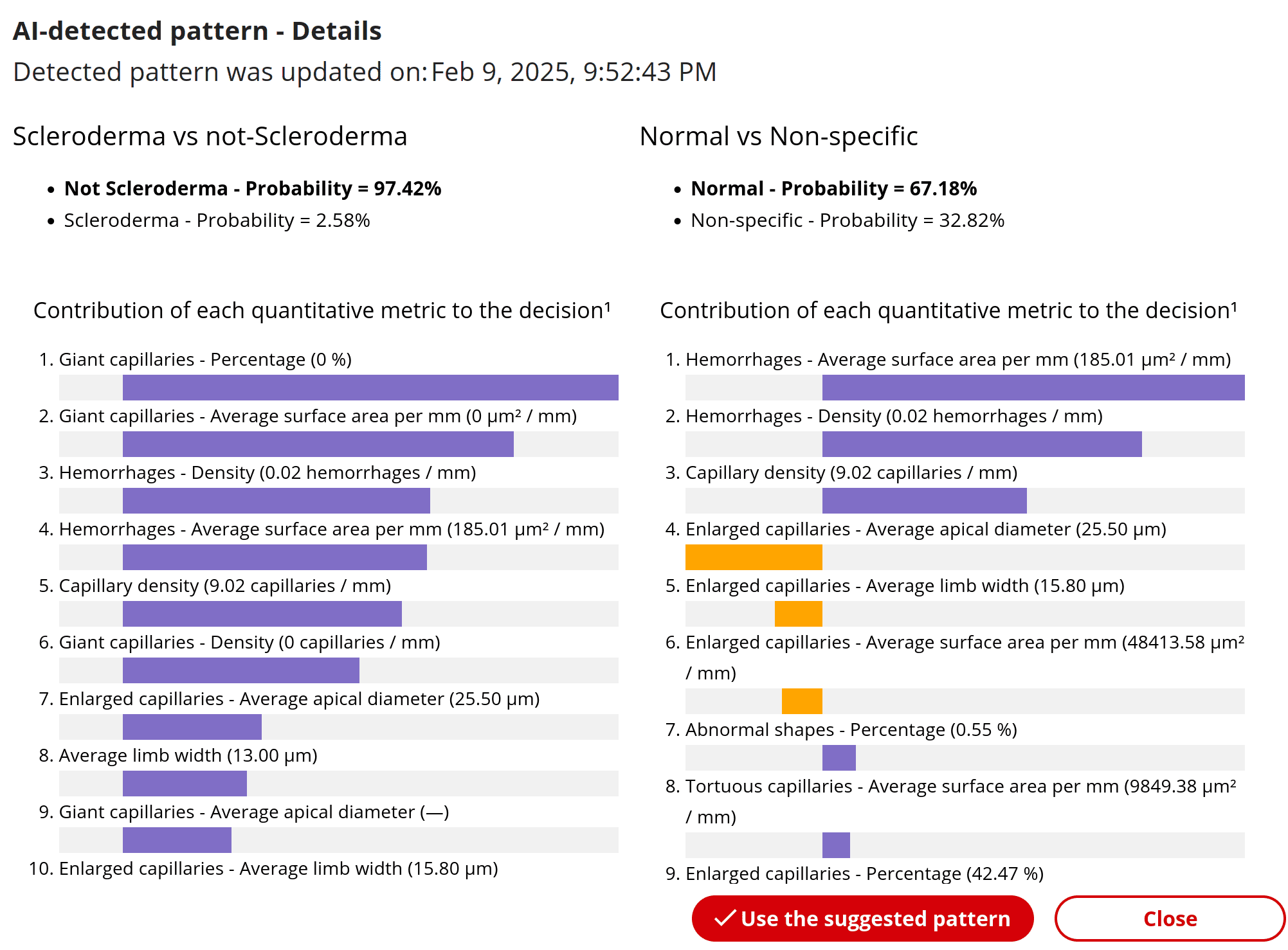
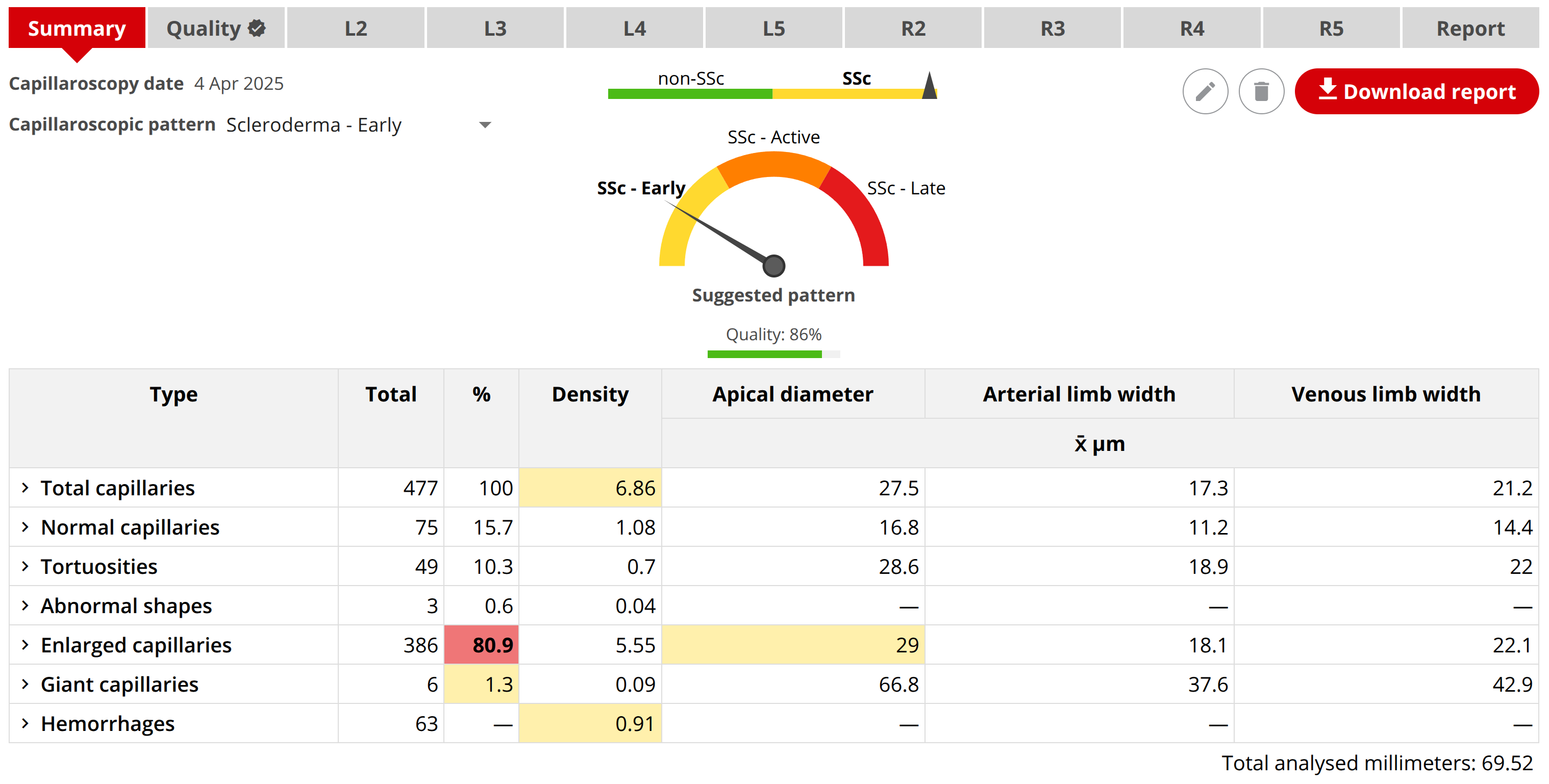
Capillary.io's own documentation adds an important operational detail: a capillaroscopy study may contain multiple images per finger, and the platform then generates an immediate quantitative report for the whole set of images, as well as an automated pattern suggestion and quality assessment [22]. This combination of rapid analysis and quality control is especially important in research, where it allows large databases to be compared, centers or batches with poorer relative quality to be detected, and large datasets to be exploited without manual image review becoming the main bottleneck [13, 20, 22].
A capillaroscopy study can group multiple images per finger and return an immediate quantitative summary with pattern suggestion and quality.
Reproducibility, Validation, and Bias
The critical variable in capillaroscopy AI is not only performance, but the reproducibility of the whole "ecosystem": image, quality assessment, labeling, algorithm, report, and clinical context [2, 3, 4, 5, 7, 8, 9, 10, 11, 12, 13].
The first bias appears in the label, that is, the diagnostic category or variable that experts assign to each image to train the model. CAPI-Score and CAPI-Detect learn from human consensus, partial or complete [8, 9]. This means the model may endorse agreement between experts without necessarily discovering a distinct biological truth. This nuance does not invalidate the method, but it does require results to be interpreted as support for consensus classification, not as a replacement for clinical medicine.
The second bias is technical. Differences in magnification, illumination, number of fingers, nailfold sectors, quality of the distal row, and confounders such as traumatic cuticle or edema can alter variable identification [2, 7, 11, 12, 13, 24]. That is why recent consensus documents insist on defining minimum variable domains to give the study validity. In 2026, the Italian group agreed to assess 23 items and considered 16 of them mandatory for reliable routine reporting [12]. The core domain set proposed in 2024 reinforces the same idea: if what is described is not harmonized, the algorithm and the human reader end up comparing different materials [11]. The purpose of automated quality control is precisely to avoid this initial risk, rather than to achieve a "magical" improvement in the final diagnosis [13].
The third bias lies in clinical translation. A model trained mainly to distinguish SSc from non-SSc may perform very well and still be of limited value in an environment dominated by borderline patterns, non-scleroderma connective tissue diseases, or poor-quality studies [8, 9, 10, 14]. The previously mentioned study on nonspecific patterns illustrates this problem well: even with 761 cases and intensive cross-validation, the F1-score did not exceed 0.632, and most errors consisted of labeling autoimmune diseases as primary Raynaud's phenomenon [14]. External validation is therefore not a "methodological luxury"; it is the minimum condition needed to give software reliability in contexts different from the environment in which it was developed [7].
Real-World Integration
The right question is not only whether AI "works and improves," but also where it fits without worsening the process. In a real laboratory or clinic, useful automation is what saves time, reduces variability, and makes clear where expert "human" judgment is still needed [1, 2, 3, 5, 7, 11, 12, 13].
The most reasonable integration can be broken down into several phases. First, acquisition. Second, quality assessment with immediate feedback to exclude invalid content and identify valid but suboptimal images [13]. Third, support for detection and quantification: count better, measure better, locate hemorrhages, or mark abnormal capillaries [6, 7]. Fourth, classification assistance: propose, with reasonable confidence, whether a study suggests a normal, nonspecific, or scleroderma pattern [8, 9, 10, 14]. Fifth, report support: complete structured domains and remind the user of confounders or mandatory fields according to existing consensus documents [11, 12].
Clinically, this dynamic reduces downtime. If a standard case includes 32 images, reviewing their quality one by one, counting capillaries, and summarizing findings can become a substantial burden even for expert teams [24]. If quality control, quantification, and summary are generated immediately, the professional can spend more time on clinical translation and less on repetitive work [13, 22]. The gain is not only convenience; it also reduces the temptation to simplify acquisition or analyze fewer fingers than desirable to relieve clinical pressure.
In research, the impact may be even greater. Rapid automation allows collections with hundreds or thousands of capillaroscopies to be exploited, subgroups compared, relative quality between centers reviewed, and invalid images filtered automatically before model training or statistical analysis [7, 13, 14, 15, 16, 17, 18, 19, 20, 22]. The main advantage is therefore not, or not only, "going faster," but being able to ask research questions that would be unfeasible if every image had to be reviewed and annotated manually from scratch.

What still does not seem acceptable is a clinical "auto-report" completely blind to acquisition quality or patient context. Even where performance is high, recent literature still keeps the expert observer as the final arbiter, especially in "borderline" diagnoses or when categories are clinically subtle [5, 8, 9, 10, 12].
| Scenario | Where AI helps | Where it should not act alone |
|---|---|---|
| High-volume Raynaud clinic | Initial screening, quality control, and structured counting [8, 9, 10, 13, 14] | Final diagnosis without clinical correlation |
| Expert systemic sclerosis center | Reduce variability, monitor quality, and accelerate quantification [7, 8, 9, 13] | Replacing expert reading in complex cases |
| Multicenter study or registry | Standardize measurements, quality control, and reporting [7, 11, 12, 13] | Combining heterogeneous data without quality control |
| Non-scleroderma diseases | Generate exploratory quantitative data and test prognostic hypotheses [14, 15, 16, 17, 18] | Applying models trained only in SSc |
Short Clinical Scenarios
Case 1. Raynaud's phenomenon with "borderline" images
A general center uses a quantitative algorithm to separate normal from nonspecific studies and detect scleroderma pattern. Before classification, the quality assessment module identifies several images because of low magnification and reflections. This alert is already clinically useful: it forces repeat acquisition before accepting, with insufficient confidence, a "non-scleroderma, nonspecific pattern" result. The sensible decision is not to accept or reject the raw result, but to review quality, apply Fast Track if appropriate, and correlate with serology and clinical evolution [3, 5, 8, 9, 13, 14].
Case 2. Multicenter inflammatory myopathy registry
A multicenter project wants to quantify hemorrhages and density in different hospitals. Here AI may contribute more than in an individual consultation because it harmonizes measurements and reduces reading burden, but it remains essential to define the acquisition protocol, quality control, and common definitions before analyzing prognostic associations. The preliminary CapIAMI data support precisely this combined approach between automated quantification and biomarkers, rather than replacement of the clinician [11, 12, 13, 15].
FAQ
Can AI replace the expert capillaroscopist?
No. It can contribute to detection, quantification, and classification, but current evidence does not support replacing expert reading in individual cases [7, 8, 9, 10, 12].
Today, what problem does automation solve best?
Reducing part of the variability in detecting capillaries, measuring structured domains, and supporting classification of scleroderma versus non-scleroderma pattern [3, 6, 7, 8, 9].
Where does it still fail most?
In "borderline" categories such as normal versus nonspecific pattern, poor-quality images, and transfer of models to different populations, devices, or centers [5, 7, 8, 9, 10].
Are CAPI-Score and CAPI-Detect the same?
No. CAPI-Score uses relatively simple quantitative rules; CAPI-Detect uses machine learning with more architectural variables [8, 9].
Does the Capillary.io platform have peer-reviewed publications?
Yes. The Capillary.io publications page lists peer-reviewed articles and conference abstracts; nevertheless, each study should be judged by its design, validation, and real clinical utility, not by the platform brand [6, 7, 8, 9, 13, 14, 15, 16, 17, 18, 19, 20].
Glossary
- Quantification
- Conversion of capillaroscopic findings into measurable, continuous, or categorical variables that can be compared between observers or centers.
- External validation
- Assessment of an algorithm's validity using data different from those used to develop it, ideally from other centers, devices, or populations.
- Fast Track
- Simplified algorithm proposed by EULAR to quickly differentiate scleroderma pattern from non-scleroderma pattern.
- CAPI-Score
- Rule-based quantitative algorithm that classifies capillaroscopic patterns using variables such as density, giant capillaries, abnormal capillaries, tortuosities, and hemorrhages.
- CAPI-Detect
- Machine-learning model that incorporates a larger number of architectural variables to improve capillaroscopic pattern classification.
- Quality assessment
- Automatic or manual evaluation of whether an image has enough quality to enter analysis, including detection of poor focus, reflections, incorrect magnification, or invalid content.
References
- Smith V, Cutolo M, Herrick AL, Ingegnoli F, Ruaro B, Sulli A, et al. Nailfold capillaroscopy. Best Pract Res Clin Rheumatol. 2023;37(1):101849. DOI: 10.1016/j.berh.2023.101849. PMID: 37419757.
- Smith V, Herrick AL, Ingegnoli F, Damjanov N, De Angelis R, Denton CP, et al. Standardisation of nailfold capillaroscopy for the assessment of patients with Raynaud's phenomenon and systemic sclerosis. Autoimmun Rev. 2020;19(3):102458. DOI: 10.1016/j.autrev.2020.102458. PMID: 31927087.
- Smith V, Vanhaecke A, Herrick AL, Distler O, Guerra MG, Denton CP, et al. Fast track algorithm: How to differentiate a "scleroderma pattern" from a "non-scleroderma pattern". Autoimmun Rev. 2019;18(11):102394. DOI: 10.1016/j.autrev.2019.102394. PMID: 31520797.
- Dinsdale G, Murray A, Moore T, Manning J, Wilkinson J, Herrick AL. Intra-and inter-observer reliability of nailfold videocapillaroscopy - A possible outcome measure for systemic sclerosis-related microangiopathy. Microvasc Res. 2017;112:1-6. DOI: 10.1016/j.mvr.2017.02.001. PMID: 28163035.
- Ng SA, Tan WH, Saffari SE, Low AHL. Evaluation of Nailfold Capillaroscopy Online Training Using the Fast Track Algorithm. J Rheumatol. 2023;50(3):368-372. DOI: 10.3899/jrheum.220794. PMID: 36455942.
- Gracia Tello B, Ramos Ibañez E, Fanlo Mateo P, Sáez Cómet L, Martínez Robles E, Ríos Blanco JJ, et al. The challenge of comprehensive nailfold videocapillaroscopy practice: a further contribution. Clin Exp Rheumatol. 2022;40(10):1926-1932. DOI: 10.55563/clinexprheumatol/6usce8. PMID: 34936544.
- Gracia-Tello B, Sáez-Comet L, Lledó G, Freire Dapena M, Guillén del Castillo A, Simeón-Aznar CP, et al. External clinical validation of automated software to identify structural abnormalities and microhaemorrhages in nailfold videocapillaroscopy images. Clin Exp Rheumatol. 2023;41(8):1605-1611. DOI: 10.55563/clinexprheumatol/4y38g6. PMID: 37140670.
- Gracia Tello BC, Sáez Comet L, Lledó G, Freire Dapena M, Mesa MA, Martín-Cascón M, et al. CAPI-Score: a quantitative algorithm for identifying disease patterns in nailfold videocapillaroscopy. Rheumatology (Oxford). 2024;63(12):3315-3321. DOI: 10.1093/rheumatology/keae197. PMID: 38530791.
- Lledó-Ibáñez GM, Sáez Comet L, Freire Dapena M, Mesa Navas M, Martín Cascón M, Guillén Del Castillo A, et al. CAPI-Detect: machine learning in capillaroscopy reveals new variables influencing diagnosis. Rheumatology (Oxford). 2025;64(6):3667-3675. DOI: 10.1093/rheumatology/keaf073. PMID: 39918978.
- Garaiman A, Nooralahzadeh F, Mihai C, Perez Gonzalez N, Gkikopoulos N, Becker MO, et al. Vision transformer assisting rheumatologists in screening for capillaroscopy changes in systemic sclerosis: an artificial intelligence model. Rheumatology (Oxford). 2023;62(7):2492-2500. DOI: 10.1093/rheumatology/keac541. PMID: 36347487.
- El Miedany Y, Ismail S, Wadie M, Müller-Ladner U, Giacomelli R, Liakouli V, et al. Development of a core domain set for nailfold capillaroscopy reporting. Reumatol Clin (Engl Ed). 2024;20(7):345-352. DOI: 10.1016/j.reumae.2024.07.003. PMID: 39160005.
- Ingegnoli F, Pireddu D, Platania E, De Angelis R, Alunno A, Ariani A, et al. Clinical practice guidelines for reporting nail fold videocapillaroscopy: a Delphi consensus on behalf of the Italian Society of Rheumatology study group on capillaroscopy. Clin Exp Rheumatol. 2026 Jan 15. Online ahead of print. DOI: 10.55563/clinexprheumatol/2z4j95. PMID: 41537537.
- Gracia Tello B, Lledó Ibáñez G, Sáez Comet L, Ramos ibáñez E. Automated Feedback and Quality Control in Nailfold Capillaroscopy: A Tool for Clinical and Educational Use [abstract]. Arthritis Rheumatol. 2025;77(suppl 9). Available at: https://acrabstracts.org/abstract/automated-feedback-and-quality-control-in-nailfold-capillaroscopy-a-tool-for-clinical-and-educational-use/
- Maldonado G, Marin Ballve A, Sáez Comet L, Freire Dapena M, Mesa M, Martín Cascón M, et al. Machine Learning-Based Classification of Raynaud's Phenomenon and Autoimmune Diseases in Indeterminate Capillaroscopic Patterns [abstract]. Arthritis Rheumatol. 2025;77(suppl 9). Available at: https://acrabstracts.org/abstract/machine-learning-based-classification-of-raynauds-phenomenon-and-autoimmune-diseases-in-indeterminate-capillaroscopic-patterns/
- Lledó Ibáñez G, Álvarez-Troncoso J, Gracia Tello B, Prieto-Gonzalez S, Martínez Robles E, Cristina-Varela D, et al. Artificial Intelligence-Based Capillaroscopy and Laboratory Biomarkers to Predict Disease Activity in Idiopathic Inflammatory Myopathies: Preliminary Data from the CapIAMI Cohort [abstract]. Arthritis Rheumatol. 2025;77(suppl 9). Available at: https://acrabstracts.org/abstract/artificial-intelligence-based-capillaroscopy-and-laboratory-biomarkers-to-predict-disease-activity-in-idiopathic-inflammatory-myopathies-preliminary-data-from-the-capiami-cohort/
- Carrillo M, Bedoya-Loaiza J, Ibáñez-Antequera C, Gallego L, Escobar A, Rojas-Villarraga A, et al. Capillaroscopic Signatures in Autoimmune Rheumatic Diseases: Unveiling Patterns in Systemic Sclerosis, Polyautoimmunity, and PAH [abstract]. Arthritis Rheumatol. 2025;77(suppl 9). Available at: https://acrabstracts.org/abstract/capillaroscopic-signatures-in-autoimmune-rheumatic-diseases-unveiling-patterns-in-systemic-sclerosis-polyautoimmunity-and-pah/
- Zheng Z, Metni L, Kim S, Neely J. Evaluating Nailfold Capillary Changes as Indicators of Disease Activity in Juvenile Dermatomyositis [abstract]. Arthritis Rheumatol. 2025;77(suppl 9). Available at: https://acrabstracts.org/abstract/evaluating-nailfold-capillary-changes-as-indicators-of-disease-activity-in-juvenile-dermatomyositis/
- McClellan N, Vandenbergen S, Matossian S, Kahlenberg J, Turnier J. Differences in Nailfold Capillary Morphology Distinguish Juvenile Dermatomyositis Patients That Are Myositis-Specific Autoantibody Positive [abstract]. Arthritis Rheumatol. 2023;75(suppl 9). Available at: https://acrabstracts.org/abstract/differences-in-nailfold-capillary-morphology-distinguish-juvenile-dermatomyositis-patients-that-are-myositis-specific-autoantibody-positive/
- Capillary.io. Publications. Capillary.io; accessed March 9, 2026. Available at: https://es.capillary.io/publicaciones/
- Capillary.io. Research projects: CapIAMI. Capillary.io; accessed March 9, 2026. Available at: https://es.capillary.io/investigacion/
- Tanidir IC, Caglayan D, Delen Y, Kokturk F, Demirkol S, Cicek OF, et al. Deep Learning Performance in Analyzing Nailfold Videocapillaroscopy Images in Systemic Sclerosis. Diagnostics (Basel). 2025;15(2):205. DOI: 10.3390/diagnostics15020205. PMID: 41300936.
- Sekiyama JY, Camargo CZ, Eduardo L, Andrade CR, Kayser C. Reliability of widefield nailfold capillaroscopy and video capillaroscopy in the assessment of patients with Raynaud's phenomenon. Arthritis Care Res (Hoboken). 2013;65(11):1853-1861. DOI: 10.1002/acr.22054. PMID: 23754794.
- Capillary.io. Capillary.io features. Capillary.io; accessed March 9, 2026. Available at: https://es.capillary.io/funcionalidades/
- Guillén del Castillo A, Lledó-Ibáñez GM, Sáez Comet L, Freire Dapena M, Mesa Navas M, Martín Cascón M, et al. Value of nailfold capillaroscopy in the classification of the systemic sclerosis pattern. Med Clin (Barc). 2026;166:107426. DOI: 10.1016/j.medcli.2026.107426. PMID: 42013567.